

Review
doi: 10.1056/NEJMra0804647.
Inflammatory bowel disease
Affiliations
- PMID: 19923578
- PMCID: PMC3491806
- DOI: 10.1056/NEJMra0804647
Item in Clipboard
Review
Inflammatory bowel disease
N Engl J Med.
.
No abstract available
Figures
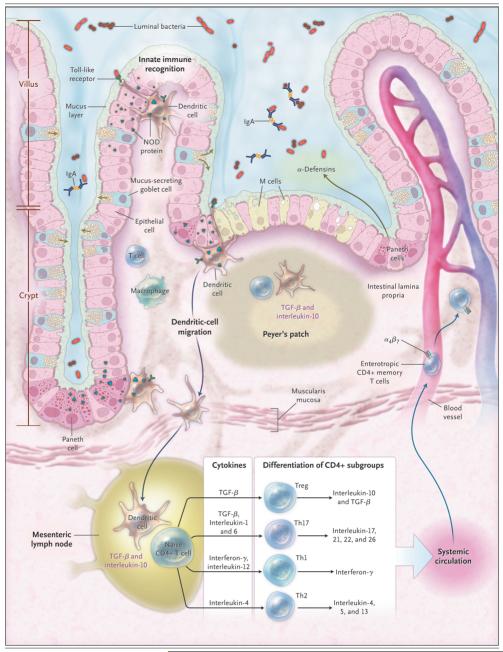
In the healthy state, the goblet cells secrete a layer of mucus that limits exposure of the intestinal epithelial cells to bacteria. Both the secretion of antimicrobial peptides (e.g., α-defensins) by Paneth cells and the production of immunoglobulin A (IgA) provide additional protection from luminal microbiota. Innate microbial sensing by epithelial cells, dendritic cells, and macrophages is mediated through pattern-recognition receptors such as toll-like receptors and nucleotide oligomerization domain (NOD) proteins. Dendritic cells present antigens to naive CD4+ T cells in secondary lymphoid organs (Peyer’s patches and mesenteric lymph nodes), where factors such as the phenotype of the antigen-presenting cells and the cytokine milieu (transforming growth factor β [TGF-β] and interleukin-10) modulate differentiation of CD4+ T-cell subgroups with characteristic cytokine profiles (regulatory T cells [e.g., Treg] and helper T cells [e.g., Th1, Th2, and Th17]), and enterotropic molecules (e.g., α4β7) are induced that provide for gut homing of lymphocytes from the systemic circulation. These activated CD4+ T cells then circulate to the intestinal lamina propria, where they carry out effector functions.
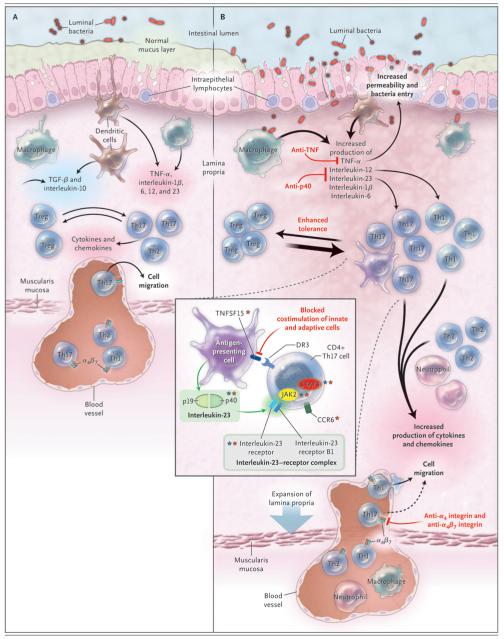
In healthy persons (Panel A), the lamina propria normally contains a diverse array of immune cells and secreted cytokines. These include antiinflammatory mediators (transforming growth factor β [TGF-β] and interleukin-10) that down-regulate immune responses, as well as proinflammatory mediators from both innate and adaptive immune cells that limit excessive entry of intestinal microbiota and defend against pathogens. Noninflammatory defenses, such as phagocytosis by macrophages, probably assist in defending against bacteria entering the lamina propria while minimizing tissue injury. A homeostatic balance is maintained between regulatory T cells (e.g., Treg) and effector T cells (Th1, Th2, and Th17). In persons with intestinal inflammation (Panel B), several events contribute to increased bacterial exposure, including disruption of the mucus layer, dysregulation of epithelial tight junctions, increased intestinal permeability, and increased bacterial adherence to epithelial cells. In inflammatory bowel disease, innate cells produce increased levels of tumor necrosis factor α (TNF-α), interleukin-1β, interleukin-6, interleukin-12, interleukin-23, and chemokines. There is marked expansion of the lamina propria, with increased numbers of CD4+ T cells, especially proinflammatory T-cell subgroups, which also secrete increased levels of cytokines and chemokines. Increased production of chemokines results in recruitment of additional leukocytes, resulting in a cycle of inflammation. At present, therapeutic approaches to inflammatory bowel disease (labels in red) focus on inhibiting proinflammatory cytokines, inhibiting the entry of cells into intestinal tissues (dashed arrow), and inhibiting T-cell activation and proliferation. Additional investigational biologic therapies include blockade of costimulatory signals that enhance interactions between innate cells and adaptive cells, administration of epithelial growth factors, and enhancement of tolerance through a variety of mechanisms. CD4+ Th17 cells (inset) express surface molecules such as the interleukin-23 receptor (a component of the interleukin-23–receptor complex, which consists of the interleukin-23 receptor and the interleukin-12 receptor B1) and CCR6. Interleukin-23 (comprising subunits p19 and p40) is secreted by antigen-presenting cells, and engagement of interleukin-23 with the interleukin-23–receptor complex results in activation of the Janus-associated kinase (JAK2) signal transducers and activators of transcription (STAT3), thereby regulating transcriptional activation. Interleukin-23 contributes to Th17-cell proliferation, survival, or both, and its actions are enhanced by tumor necrosis factor (ligand) superfamily, member 15 (TNFS15). Of the top 30 genetic associations with Crohn’s disease, at least six genes can be implicated in Th17 cells and interleukin-23 signaling. A number of these genes are not unique to interleukin-23–Th17 signaling. Genes in the interleukin-23–Th17 pathway that have been associated with Crohn’s disease are designated by red stars, and those with ulcerative colitis by blue stars.
References
-
- Hampe J, Franke A, Rosenstiel P, et al. A genome-wide association scan of non-synonymous SNPs identifies a susceptibility variant for Crohn disease in ATG16L1. Nat Genet. 2007;39:207–11. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical