

Blocking the glucocorticoid receptor with RU-486 does not prevent glucocorticoid control of autoimmune mouse hearing loss
- PMID: 19923812
- PMCID: PMC2820331
- DOI: 10.1159/000241899
Blocking the glucocorticoid receptor with RU-486 does not prevent glucocorticoid control of autoimmune mouse hearing loss
Abstract
Background/aims: Glucocorticoids effectively manage autoimmune hearing loss, although the cochlear mechanisms involved are unknown. Previous studies of steroid-responsive hearing loss in autoimmune (lupus) mice showed glucocorticoids and mineralocorticoids were equally effective, suggesting the ion homeostasis functions of glucocorticoids may be as relevant as immunosuppression for control of autoimmune-induced inner ear disease. Therefore, to better characterize the role of the glucocorticoid receptor in autoimmune hearing loss therapy, its function was blocked with the antagonist RU-486 (mifepristone) during glucocorticoid (prednisolone) treatments.
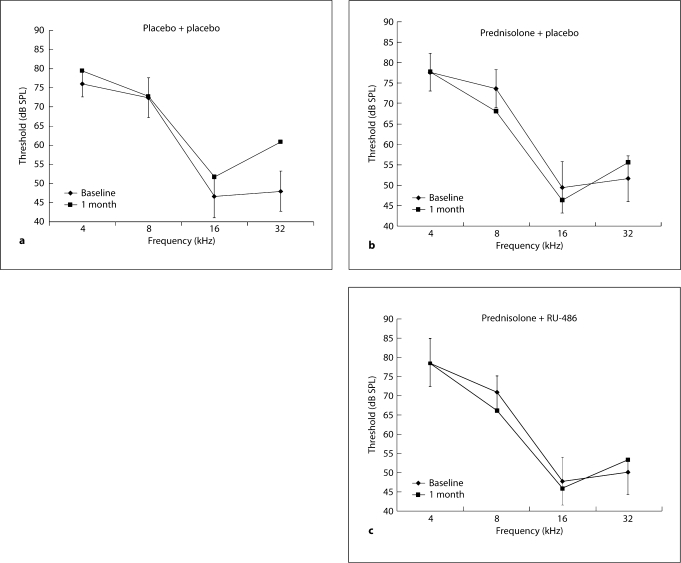
Methods: Following baseline auditory brainstem response (ABR) thresholds, MRL/MpJ-Fas(lpr) autoimmune mice were implanted with pellets providing combinations of 1.25 mg/kg of RU-486, 4 mg/kg of prednisolone, or their respective placebos. After 1 month, animals were retested with ABR and blood was collected for immune complex analyses.
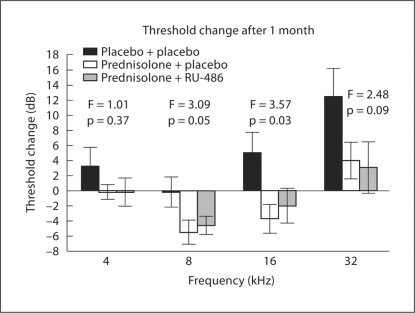
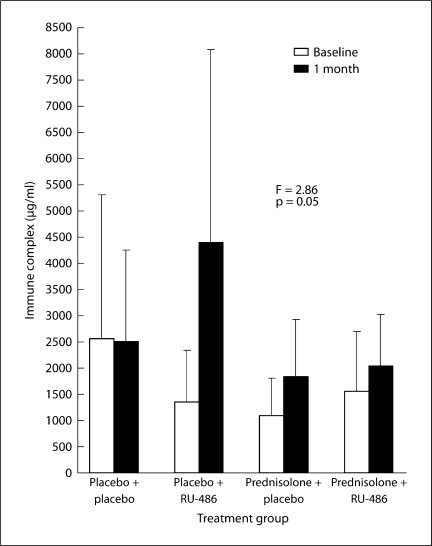
Results: Mice receiving no prednisolone (placebo + placebo and placebo + RU-486) showed continued declines in hearing. On the other hand, mice receiving prednisolone (prednisolone + placebo and prednisolone + RU-486) had significantly better hearing (p < 0.05) than the non-prednisolone groups. Immune complexes were significantly elevated in the placebo + RU-486 group, suggesting RU-486 effectively blocked glucocorticoid receptor-mediated immune suppression. These results showed that blockage of the glucocorticoid receptor with RU-486 did not prevent prednisolone's effects in the ear, suggesting its ion homeostasis actions via the mineralocorticoid receptor were more relevant in hearing control.
Conclusion: The mineralocorticoid receptor-mediated actions of glucocorticoids are potentially relevant in steroid-responsive hearing disorders, implying disrupted cochlear ion transport functions may underlie the vascular problems proposed in some forms of immune-mediated hearing loss.
(c) 2009 S. Karger AG, Basel.
Figures
Similar articles
-
Mineralocorticoid receptor mediates glucocorticoid treatment effects in the autoimmune mouse ear.Hear Res. 2006 Feb;212(1-2):22-32. doi: 10.1016/j.heares.2005.10.006. Epub 2005 Nov 22. Hear Res. 2006. PMID: 16307853
-
Aldosterone (mineralocorticoid) equivalent to prednisolone (glucocorticoid) in reversing hearing loss in MRL/MpJ-Fas1pr autoimmune mice.Laryngoscope. 2000 Nov;110(11):1902-6. doi: 10.1097/00005537-200011000-00025. Laryngoscope. 2000. PMID: 11081607
-
Steroid treatment in young MRL.MpJ-Fas(lpr) autoimmune mice prevents cochlear dysfunction.Hear Res. 1999 Nov;137(1-2):167-73. doi: 10.1016/s0378-5955(99)00148-3. Hear Res. 1999. PMID: 10545644
-
The antiglucocorticoid action of mifepristone.Pharmacol Ther. 1996;70(3):183-213. doi: 10.1016/0163-7258(96)00016-2. Pharmacol Ther. 1996. PMID: 8888066 Review.
-
Corticosteroid therapy for hearing and balance disorders.Anat Rec (Hoboken). 2012 Nov;295(11):1928-43. doi: 10.1002/ar.22576. Epub 2012 Oct 8. Anat Rec (Hoboken). 2012. PMID: 23044978 Free PMC article. Review.
Cited by
-
Low dose combination steroids control autoimmune mouse hearing loss.J Neuroimmunol. 2010 Dec 15;229(1-2):140-5. doi: 10.1016/j.jneuroim.2010.07.026. Epub 2010 Aug 30. J Neuroimmunol. 2010. PMID: 20800906 Free PMC article.
-
Utilizing Single Cell RNA-Sequencing to Implicate Cell Types and Therapeutic Targets for SSNHL in the Adult Cochlea.Otol Neurotol. 2021 Dec 1;42(10):e1410-e1421. doi: 10.1097/MAO.0000000000003356. Otol Neurotol. 2021. PMID: 34510123 Free PMC article.
-
Cortisol Sensitizes Cochlear Hair Cells to Gentamicin Ototoxicity Via Endogenous Apoptotic Pathway.Otol Neurotol. 2024 Jan 1;45(1):e49-e56. doi: 10.1097/MAO.0000000000004074. Epub 2023 Nov 26. Otol Neurotol. 2024. PMID: 38085767 Free PMC article.
-
Ion homeostasis in the ear: mechanisms, maladies, and management.Curr Opin Otolaryngol Head Neck Surg. 2010 Oct;18(5):413-9. doi: 10.1097/MOO.0b013e32833d9597. Curr Opin Otolaryngol Head Neck Surg. 2010. PMID: 20693900 Free PMC article. Review.
-
Advances in Auditory and Vestibular Medicine.Audiol Med. 2009 Dec 1;7(4):180-188. doi: 10.3109/02841860903364076. Audiol Med. 2009. PMID: 20711412 Free PMC article.
References
-
- Dornhoffer JL, Arenberg JG, Arenberg IK, Shambaugh GE., Jr Pathophysiological mechanisms in immune inner ear disease. Acta Otolaryngol (Stockh) 1997;Suppl 526:30–36. - PubMed
-
- Alexiou C, Arnold W, Fauser C, Schratzenstaller B, Gloddek B, Fuhrmann S, Lamm K. Sudden sensorineural hearing loss: does application of glucocorticoids make sense? Arch Otolaryngol Head Neck Surg. 2001;127:253–258. - PubMed
-
- Rauch SD. Intratympanic steroids for sensorineural hearing loss. Otolaryngol Clin North Am. 2004;37:1061–1074. - PubMed
-
- Aoki D, Takegoshi H, Kikuchi S. Evaluation of super-high-dose steroid therapy for sudden sensorineural hearing loss. Otolaryngol Head Neck Surg. 2006;134:783–787. - PubMed
-
- Barrs DM. Intratympanic corticosteroids for Meniere's disease and vertigo. Otolaryngol Clin North Am. 2004;37:955–972. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
