

A critical appraisal of circumferential resection margins in esophageal carcinoma
- PMID: 19924487
- PMCID: PMC2820690
- DOI: 10.1245/s10434-009-0827-4
A critical appraisal of circumferential resection margins in esophageal carcinoma
Abstract
Background: In esophageal cancer, circumferential resection margins (CRMs) are considered to be of relevant prognostic value, but a reliable definition of tumor-free CRM is still unclear. The aim of this study was to appraise the clinical prognostic value of microscopic CRM involvement and to determine the optimal limit of CRM.
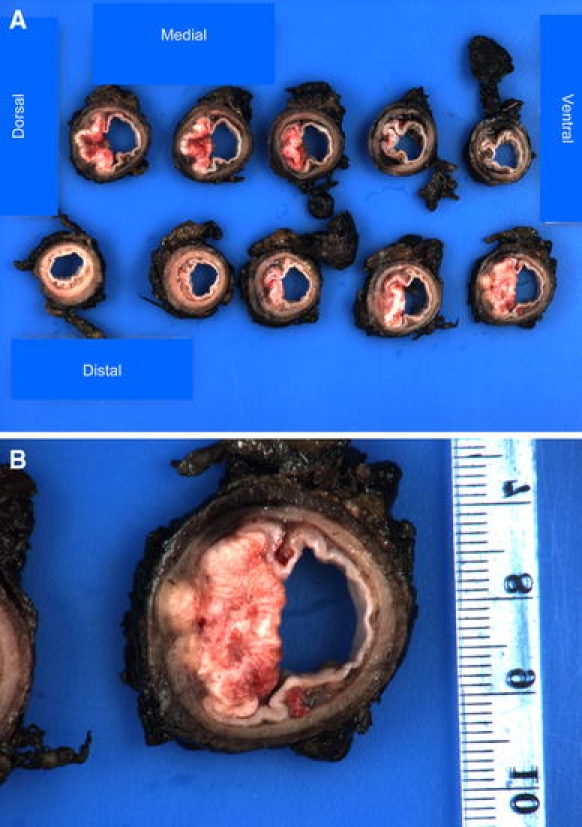
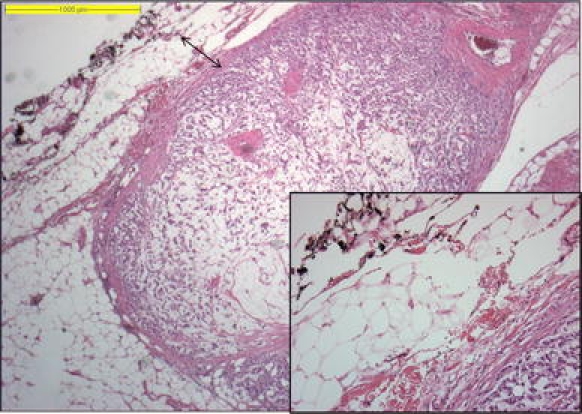
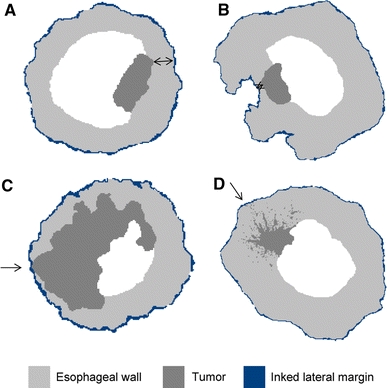
Methods: To define the optimal tumor-free CRM we included 98 consecutive patients who underwent extended esophagectomy with microscopic tumor-free resection margins (R0) between 1997 and 2006. CRMs were measured in tenths of millimeters with inked lateral margins. Outcome of patients with CRM involvement was compared with a statistically comparable control group of 21 patients with microscopic positive resection margins (R1).
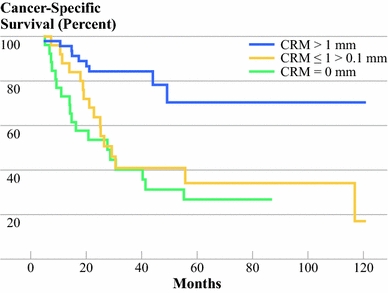
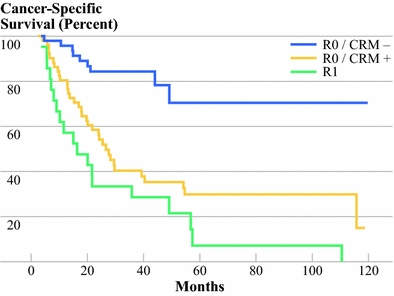
Results: A cutoff point of CRM at < or = 1.0 mm and > 1.0 mm appeared to be an adequate marker for survival and prognosis (both P < 0.001). The outcome in patients with CRMs < or = 1.0 and > 0 mm was equal to that in patients with CRM of 0 mm (P = 0.43). CRM involvement was an independent prognostic factor for both recurrent disease (P = 0.001) and survival (P < 0.001). Survival of patients with positive CRMs (< or = 1 mm) did not significantly differ from patients with an R1 resection (P = 0.12).
Conclusion: Involvement of the circumferential resection margins is an independent prognostic factor for recurrent disease and survival in esophageal cancer. The optimal limit for a positive CRM is < or = 1 mm and for a free CRM is >1.0 mm. Patients with unfavorable CRM should be approached as patients with R1 resection with corresponding outcome.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
