

Hemicraniectomy: a new model for human electrophysiology with high spatio-temporal resolution
- PMID: 19925193
- PMCID: PMC2888789
- DOI: 10.1162/jocn.2009.21384
Hemicraniectomy: a new model for human electrophysiology with high spatio-temporal resolution
Abstract
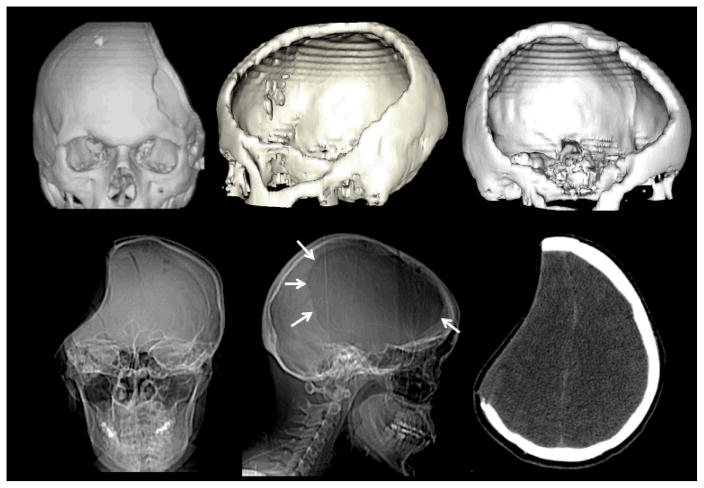
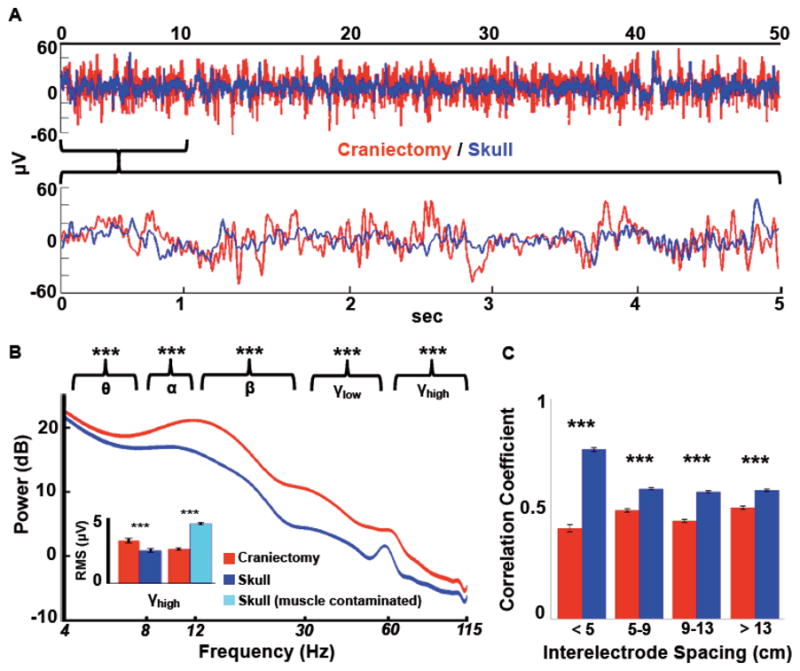
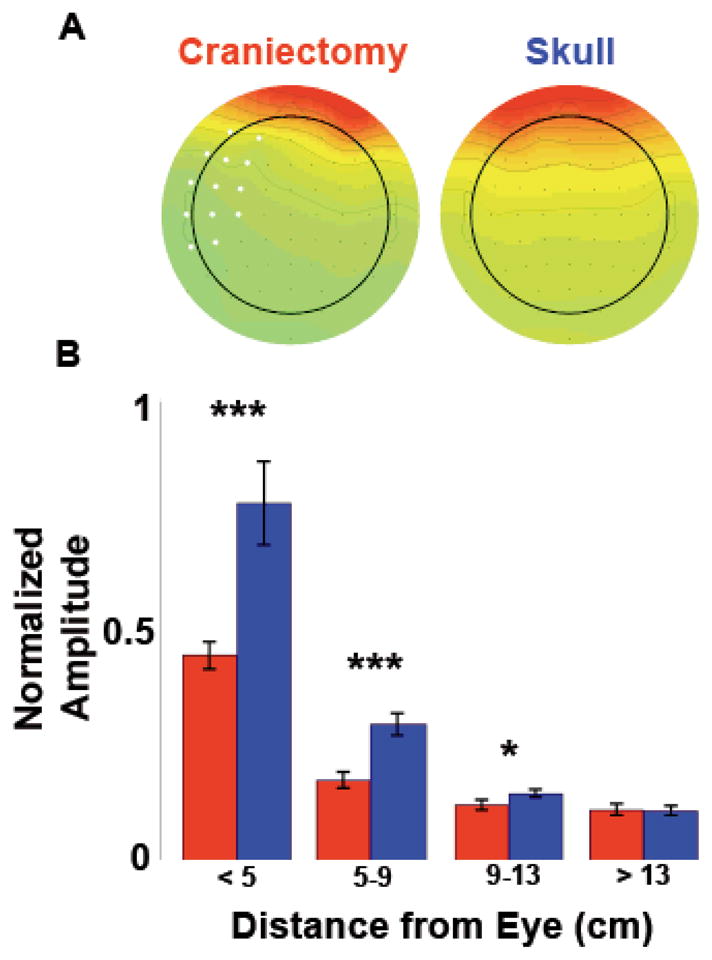
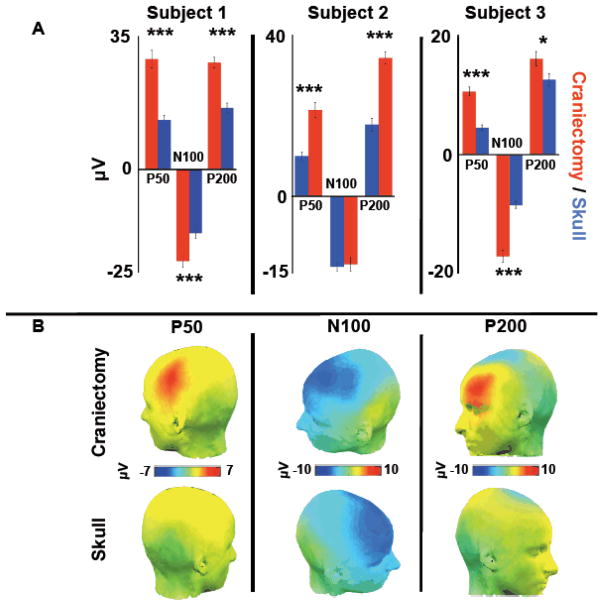
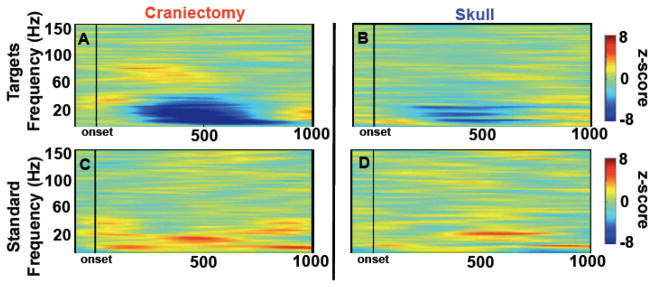
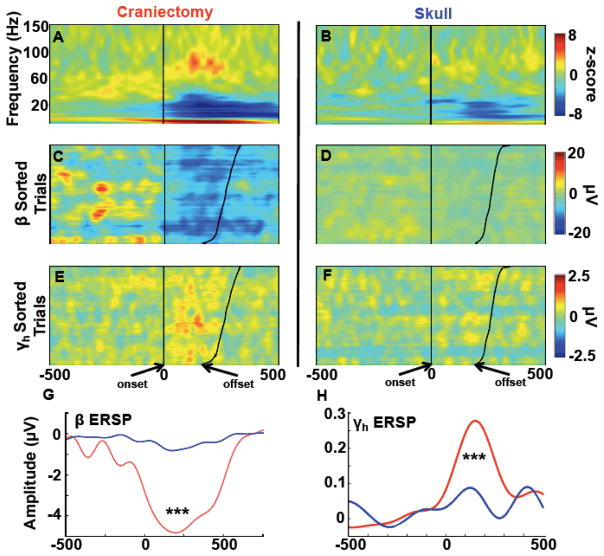
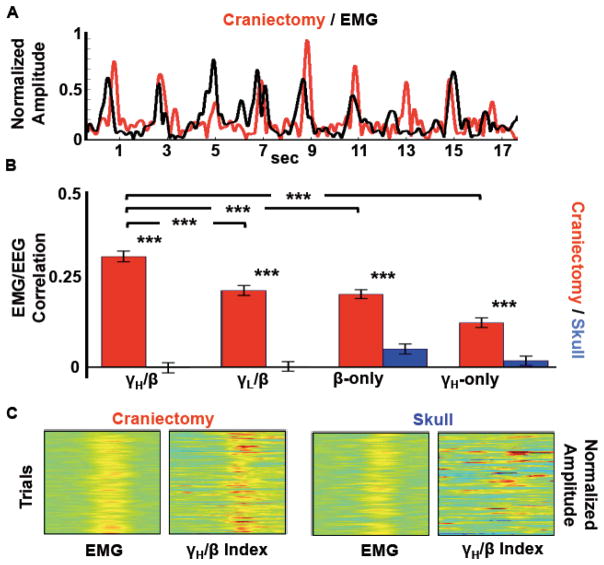
Human electrophysiological research is generally restricted to scalp EEG, magneto-encephalography, and intracranial electrophysiology. Here we examine a unique patient cohort that has undergone decompressive hemicraniectomy, a surgical procedure wherein a portion of the calvaria is removed for several months during which time the scalp overlies the brain without intervening bone. We quantify the differences in signals between electrodes over areas with no underlying skull and scalp EEG electrodes over the intact skull in the same subjects. Signals over the hemicraniectomy have enhanced amplitude and greater task-related power at higher frequencies (60-115 Hz) compared with signals over skull. We also provide evidence of a metric for trial-by-trial EMG/EEG coupling that is effective over the hemicraniectomy but not intact skull at frequencies >60 Hz. Taken together, these results provide evidence that the hemicraniectomy model provides a means for studying neural dynamics in humans with enhanced spatial and temporal resolution.
Figures
References
-
- Abraham K, Marsan C. Patterns of cortical discharges and their relation to routine scalp electroencephalography. Electroencephalography and Clinical Neurophysiology. 1958;10(3):447–461. - PubMed
-
- Ball T, Demandt E, Mutschler I, Neitzel E, Mehring C, Vogt K, Aertsen A, Schulzebonhage A. Movement related activity in the high gamma range of the human EEG. NeuroImage. 2008;41(2):302–310. - PubMed
-
- Ball T, Kern M, Mutschler I, Aertsen A, Schulze-Bonhage A. Signal quality of simultaneously recorded invasive and non-invasive EEG. NeuroImage. 2009;46 (3):708–716. - PubMed
-
- Bédard C, Kröger H, Destexhe A. Does the 1/f frequency scaling of brain signals reflect self-organized critical states? Physical Review Letters. 2006;97(11):11802-1–4. - PubMed
-
- Bénar CG, Gotman J. Modeling of post-surgical brain and skull defects in the EEG inverse problem with the boundary element method. Clinical Neurophysiology. 2002;113(1):48–56. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources