

Mycophenolate pharmacokinetics and association with response to acute graft-versus-host disease treatment from the Blood and Marrow Transplant Clinical Trials Network
- PMID: 19925875
- PMCID: PMC3104501
- DOI: 10.1016/j.bbmt.2009.11.010
Mycophenolate pharmacokinetics and association with response to acute graft-versus-host disease treatment from the Blood and Marrow Transplant Clinical Trials Network
Abstract
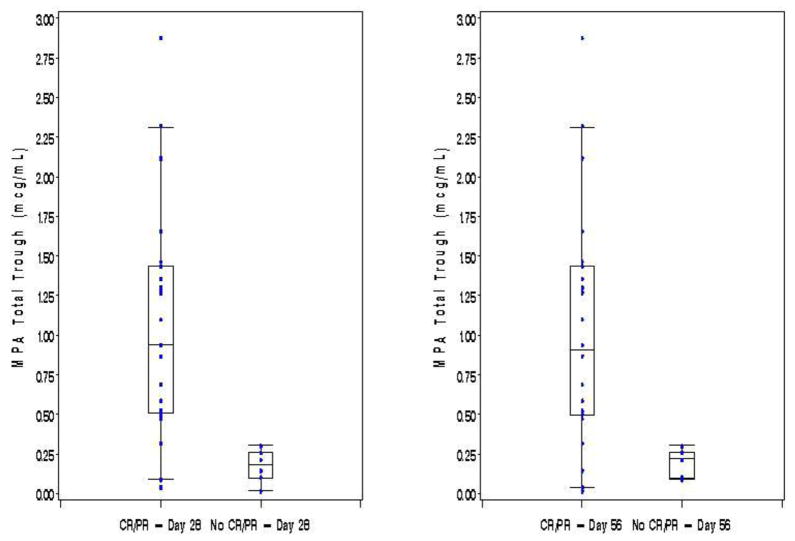
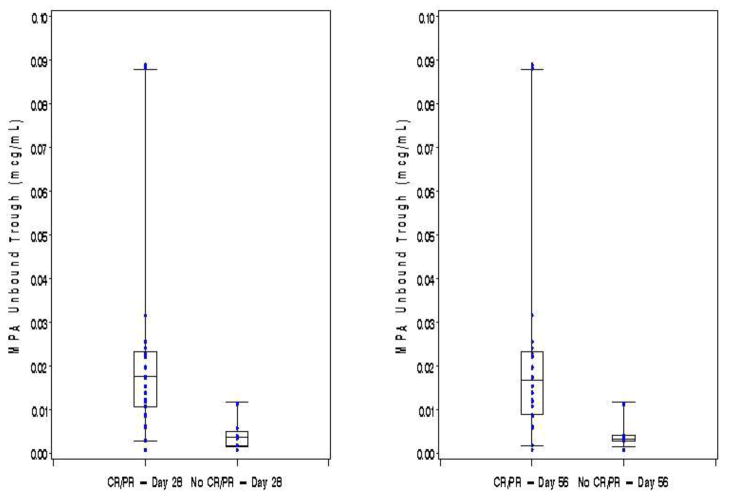
There are limited data as to the effectiveness of mycophenolate mofetil (MMF) plus high-dose corticosteroids for the treatment of acute graft-versus-host disease (aGVHD), and even less data regarding the pharmacokinetic disposition and exposure-response relationship of MMF in individuals with GVHD. MMF pharmacokinetics were studied in a multicenter Blood and Marrow Transplant Clinical Trials Network randomized phase II trial evaluating the effectiveness of MMF as one of 4 agents added to corticosteroids as treatment of aGVHD. Thirty-two of the patients randomized to receive MMF underwent pharmacokinetic sampling in weeks 1 and 2 were studied. Mean age was 41 +/- 13.6 years. Twenty one (65.6%), 5 (15.6%), 6 (18.8%) patients had a complete response (CR), partial response (PR) or lesser response by day 28, respectively. Twenty-five (78.1%), 2 (6.3%), 5 (15.6%) patients had a CR, PR, or other response by day 56 to treatment, respectively. Mycophenolic acid (MPA) pharmacokinetic measurements from weeks 1 and 2 did not correlate with CR at either day 28 or day 56 (P > .07); however, if the mean of weeks 1 and 2 total MPA troughs was >0.5 microg/mL or that of an unbound trough was >0.015 microg/mL, then a significantly greater proportion achieved CR + PR at days 28 and 56. CR + PR at day 28 was observed in 19 of 19 patients (100%) with a mean total trough >0.5 mg/mL, but in only 7 of 13 (54%) with a mean total trough < or =0.5 microg/mL (P = .002). Similarly, CR + PR at day 28 was seen in 15 of 15 patients (100%) with an unbound trough concentration >0.015 microg/mL, but in only 11 of 17 (65%) with an unbound trough concentration < or =0.015 microg/mL (P = .02). There was no association between the pharmacokinetic measures and risk of infection by day 90 or overall survival (OS) at day 180 postrandomization. About one-half of subjects did not achieve the favorable MPA total and unbound trough concentrations. The current practice of MMF 1 gm twice daily dosing provides low plasma concentrations in many patients. Higher doses may improve the efficacy of MMF as aGVHD therapy.
Trial registration: ClinicalTrials.gov NCT00224874.
Copyright (c) 2010 American Society for Blood and Marrow Transplantation. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Pharmacokinetics, efficacy, and safety of mycophenolate mofetil in combination with standard-dose or reduced-dose tacrolimus in liver transplant recipients.Liver Transpl. 2009 Feb;15(2):136-47. doi: 10.1002/lt.21657. Liver Transpl. 2009. PMID: 19177449 Clinical Trial.
-
Intensified Mycophenolate Mofetil Dosing and Higher Mycophenolic Acid Trough Levels Reduce Severe Acute Graft-versus-Host Disease after Double-Unit Cord Blood Transplantation.Biol Blood Marrow Transplant. 2015 May;21(5):920-5. doi: 10.1016/j.bbmt.2015.01.024. Epub 2015 Feb 14. Biol Blood Marrow Transplant. 2015. PMID: 25687796 Free PMC article. Clinical Trial.
-
Limited sampling models and Bayesian estimation for mycophenolic acid area under the curve prediction in stable renal transplant patients co-medicated with ciclosporin or sirolimus.Clin Pharmacokinet. 2009;48(11):745-58. doi: 10.2165/11318060-000000000-00000. Clin Pharmacokinet. 2009. PMID: 19817503
-
Mycophenolate, clinical pharmacokinetics, formulations, and methods for assessing drug exposure.Transplant Rev (Orlando). 2011 Apr;25(2):47-57. doi: 10.1016/j.trre.2010.06.001. Epub 2010 Dec 28. Transplant Rev (Orlando). 2011. PMID: 21190834
-
Mycophenolate mofetil for solid organ transplantation: does the evidence support the need for clinical pharmacokinetic monitoring?Ther Drug Monit. 2003 Apr;25(2):137-57. doi: 10.1097/00007691-200304000-00003. Ther Drug Monit. 2003. PMID: 12657908 Review.
Cited by
-
Nonrelapse mortality and mycophenolic acid exposure in nonmyeloablative hematopoietic cell transplantation.Biol Blood Marrow Transplant. 2013 Aug;19(8):1159-66. doi: 10.1016/j.bbmt.2013.04.026. Epub 2013 May 6. Biol Blood Marrow Transplant. 2013. PMID: 23660171 Free PMC article.
-
Inferior Outcomes with Cyclosporine and Mycophenolate Mofetil after Myeloablative Allogeneic Hematopoietic Cell Transplantation.Biol Blood Marrow Transplant. 2019 Sep;25(9):1744-1755. doi: 10.1016/j.bbmt.2019.05.019. Epub 2019 May 31. Biol Blood Marrow Transplant. 2019. PMID: 31158502 Free PMC article.
-
A novel reduced-intensity conditioning regimen induces a high incidence of sustained donor-derived neutrophil and platelet engraftment after double-unit cord blood transplantation.Biol Blood Marrow Transplant. 2013 May;19(5):799-803. doi: 10.1016/j.bbmt.2013.02.007. Epub 2013 Feb 14. Biol Blood Marrow Transplant. 2013. PMID: 23416850 Free PMC article.
-
Adverse events in second- and third-line treatments for acute and chronic graft-versus-host disease: systematic review.Ther Adv Hematol. 2020 Dec 8;11:2040620720977039. doi: 10.1177/2040620720977039. eCollection 2020. Ther Adv Hematol. 2020. PMID: 33343855 Free PMC article. Review.
-
Optimizing drug therapy in pediatric SCT: focus on pharmacokinetics.Bone Marrow Transplant. 2015 Feb;50(2):165-72. doi: 10.1038/bmt.2014.235. Epub 2014 Oct 27. Bone Marrow Transplant. 2015. PMID: 25347008 Free PMC article. Review.
References
-
- Martin PJ, Schoch G, Fisher L, Byers V, Anasetti C, Appelbaum FR, et al. A retrospective analysis of therapy for acute graft-versus-host disease: initial treatment. Blood. 1990;76(8):1464–1472. - PubMed
-
- Cragg L, Blazar BR, Defor T, Kolatker N, Miller W, Kersey J, et al. A randomized trial comparing prednisone with antithymocyte globulin/prednisone as an initial systemic therapy for moderately severe acute graft-versus-host disease. Biol Blood Marrow Transplant. 2000;6(4A):441–447. - PubMed
-
- Van Lint MT, Uderzo C, Locasciulli A, Majolino I, Scime R, Locatelli F, et al. Early treatment of acute graft-versus-host disease with high- or low-dose 6-methylprednisolone: a multicenter randomized trial from the Italian Group for Bone Marrow Transplantation. Blood. 1998;92(7):2288–2293. - PubMed
-
- Martin PJ, Nelson BJ, Appelbaum FR, Anasetti C, Deeg HJ, Hansen JA, et al. Evaluation of a CD5-specific immunotoxin for treatment of acute graft-versus-host disease after allogeneic marrow transplantation. Blood. 1996;88(3):824–830. - PubMed
-
- Mayer J, Krejci M, Doubek M, Pospisil Z, Brychtova Y, Tomiska M, et al. Pulse cyclophosphamide for corticosteroid-refractory graft-versus-host disease. Bone Marrow Transplant. 2005;35(7):699–705. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
