

Sodium bicarbonate plus N-acetylcysteine prophylaxis: a meta-analysis
- PMID: 19926054
- PMCID: PMC6643289
- DOI: 10.1016/j.jcin.2009.07.015
Sodium bicarbonate plus N-acetylcysteine prophylaxis: a meta-analysis
Abstract
Objectives: We sought to conduct a meta-analysis to compare N-acetylcysteine (NAC) in combination with sodium bicarbonate (NaHCO(3)) for the prevention of contrast-induced acute kidney injury (AKI).
Background: Contrast-induced AKI is a serious consequence of cardiac catheterizations and percutaneous coronary interventions (PCI). Despite recent supporting evidence for combination therapy, not enough has been done to prevent the occurrence of contrast-induced AKI prophylactically.
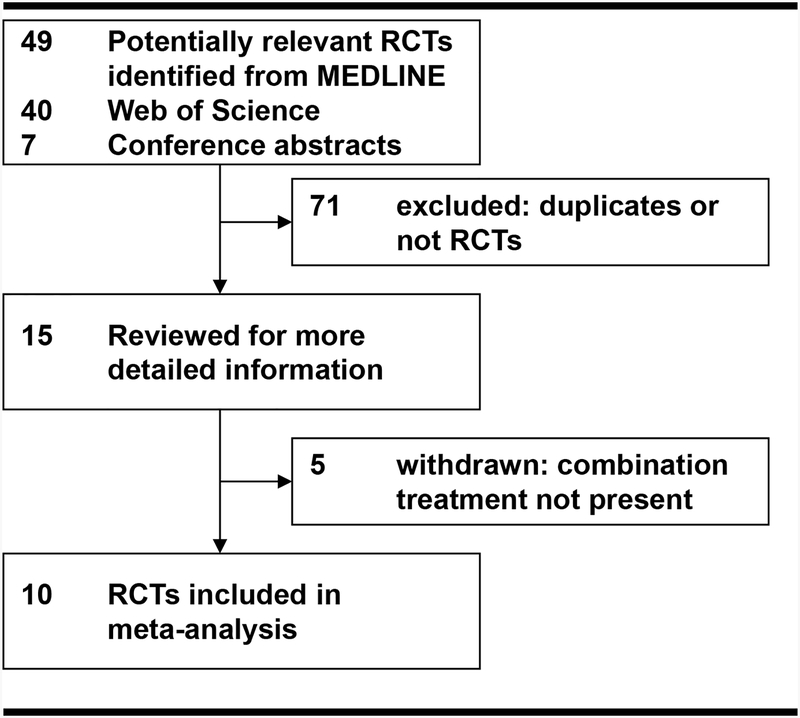
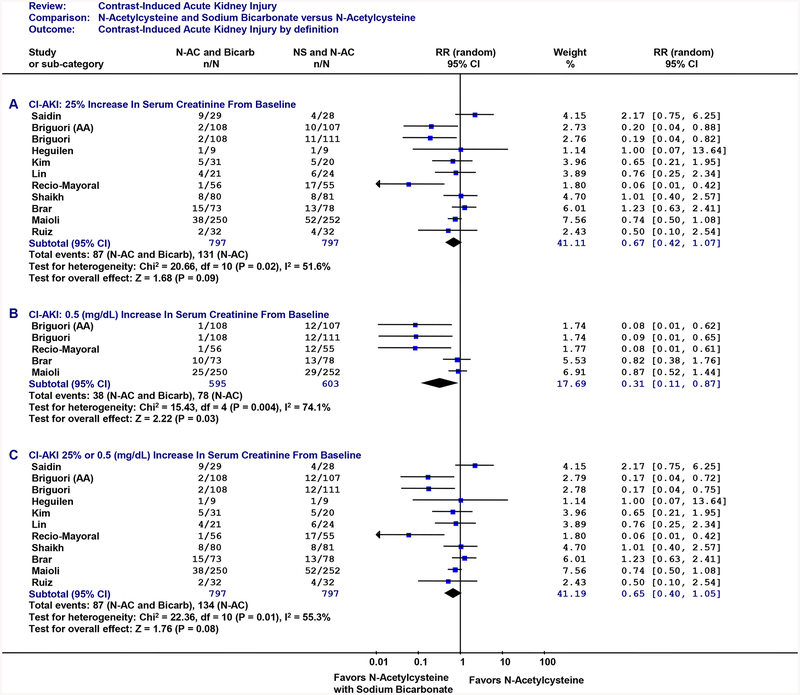
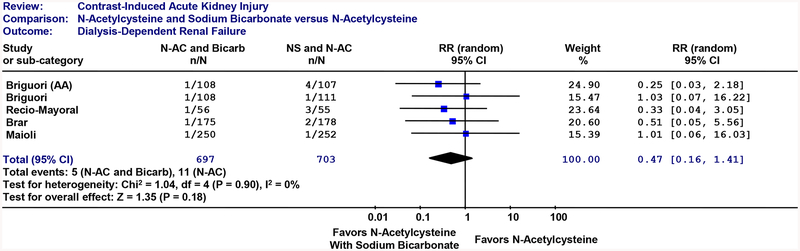
Methods: Published randomized controlled trial data were collected from OVID/PubMed, Web of Science, and conference abstracts. The outcome of interest was contrast-induced AKI, defined as a >or=25% or >or=0.5 mg/dl increase in serum creatinine from baseline. Secondary outcome was renal failure requiring dialysis.
Results: Ten randomized controlled trials met our criteria. Combination treatment of NAC with intravenous NaHCO(3) reduced contrast-induced AKI by 35% (relative risk: 0.65; 95% confidence interval: 0.40 to 1.05). However, the combination of N-acetylcysteine plus NaHCO(3) did not significantly reduce renal failure requiring dialysis (relative risk: 0.47; 95% confidence interval: 0.16 to 1.41).
Conclusions: Combination prophylaxis with NAC and NaHCO(3) substantially reduced the occurrence of contrast-induced AKI overall but not dialysis-dependent renal failure. Combination prophylaxis should be incorporated for all high-risk patients (emergent cases or patients with chronic kidney disease) and should be strongly considered for all interventional radio-contrast procedures.
Conflict of interest statement
Disclosures
There are no conflicts of interest to disclose.
Figures
Comment on
-
In search of an algorithm to prevent acute kidney injury.JACC Cardiovasc Interv. 2009 Nov;2(11):1125-7. doi: 10.1016/j.jcin.2009.08.019. JACC Cardiovasc Interv. 2009. PMID: 19926055 No abstract available.
Similar articles
-
Prevention of contrast-induced acute kidney injury in patients with stable chronic renal disease undergoing elective percutaneous coronary and peripheral interventions: randomized comparison of two preventive strategies.Catheter Cardiovasc Interv. 2012 May 1;79(6):929-37. doi: 10.1002/ccd.23148. Epub 2011 Dec 8. Catheter Cardiovasc Interv. 2012. PMID: 21542114 Clinical Trial.
-
In search of an algorithm to prevent acute kidney injury.JACC Cardiovasc Interv. 2009 Nov;2(11):1125-7. doi: 10.1016/j.jcin.2009.08.019. JACC Cardiovasc Interv. 2009. PMID: 19926055 No abstract available.
-
Comparison of short-term infusion regimens of N-acetylcysteine plus intravenous fluids, sodium bicarbonate plus intravenous fluids, and intravenous fluids alone for prevention of contrast-induced nephropathy in the emergency department.Acad Emerg Med. 2014 Jun;21(6):615-22. doi: 10.1111/acem.12400. Acad Emerg Med. 2014. PMID: 25039544 Clinical Trial.
-
Prevention of contrast-induced AKI: a review of published trials and the design of the prevention of serious adverse events following angiography (PRESERVE) trial.Clin J Am Soc Nephrol. 2013 Sep;8(9):1618-31. doi: 10.2215/CJN.11161012. Epub 2013 May 9. Clin J Am Soc Nephrol. 2013. PMID: 23660180 Free PMC article. Review.
-
The efficacy of N-acetylcysteine plus sodium bicarbonate in the prevention of contrast-induced nephropathy after cardiac catheterization and percutaneous coronary intervention: A meta-analysis of randomized controlled trials.Int J Cardiol. 2016 Oct 15;221:251-9. doi: 10.1016/j.ijcard.2016.07.086. Epub 2016 Jul 5. Int J Cardiol. 2016. PMID: 27404685 Review.
Cited by
-
Prevention and management of contrast-induced acute kidney injury.Curr Treat Options Cardiovasc Med. 2012 Feb;14(1):1-7. doi: 10.1007/s11936-011-0162-5. Curr Treat Options Cardiovasc Med. 2012. PMID: 22198848
-
Different interventions in preventing contrast-induced nephropathy after percutaneous coronary intervention.Int Urol Nephrol. 2014 Sep;46(9):1801-7. doi: 10.1007/s11255-014-0765-3. Epub 2014 Jun 26. Int Urol Nephrol. 2014. PMID: 24966097 Clinical Trial.
-
Acute kidney injury in the perioperative period and in intensive care units (excluding renal replacement therapies).Ann Intensive Care. 2016 Dec;6(1):48. doi: 10.1186/s13613-016-0145-5. Epub 2016 May 27. Ann Intensive Care. 2016. PMID: 27230984 Free PMC article. Review.
-
Acute Kidney Injury Risk Prediction in Patients Undergoing Coronary Angiography in a National Veterans Health Administration Cohort With External Validation.J Am Heart Assoc. 2015 Dec 11;4(12):e002136. doi: 10.1161/JAHA.115.002136. J Am Heart Assoc. 2015. PMID: 26656858 Free PMC article.
-
Contrast-induced acute kidney injury: the at-risk patient and protective measures.Curr Cardiol Rep. 2010 Sep;12(5):440-5. doi: 10.1007/s11886-010-0129-2. Curr Cardiol Rep. 2010. PMID: 20640537 Review.
References
-
- Bui KL, Horner JD, Herts BR, Einstein DM. Intravenous iodinated contrast agents: risks and problematic situations. Cleve Clin J Med 2007;74:361–4, 367. - PubMed
-
- Tumlin J, Stacul F, Adam A, et al. Pathophysiology of contrast-induced nephropathy. Am J Cardiol 2006;98:14K–20K. - PubMed
-
- Levy EM, Viscoli CM, Horwitz RI. The effect of acute renal failure on mortality. A cohort analysis. JAMA 1996;275:1489–94. - PubMed
-
- Gruberg L, Mintz GS, Mehran R, et al. The prognostic implications of further renal function deterioration within 48 h of interventional coronary procedures in patients with pre-existent chronic renal insufficiency. J Am Coll Cardiol 2000;36:1542–8. - PubMed
-
- McCullough PA, Adam A, Becker CR, et al. Epidemiology and prognostic implications of contrast-induced nephropathy. Am J Cardiol 2006;98:5K–13K. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
