

Predicting risk of osteoporotic fracture in men and women in England and Wales: prospective derivation and validation of QFractureScores
- PMID: 19926696
- PMCID: PMC2779855
- DOI: 10.1136/bmj.b4229
Predicting risk of osteoporotic fracture in men and women in England and Wales: prospective derivation and validation of QFractureScores
Abstract
Objective: To develop and validate two new fracture risk algorithms (QFractureScores) for estimating the individual risk of osteoporotic fracture or hip fracture over 10 years.
Design: Prospective open cohort study with routinely collected data from 357 general practices to develop the scores and from 178 practices to validate the scores.
Setting: General practices in England and Wales.
Participants: 1 183 663 women and 1 174 232 men aged 30-85 in the derivation cohort, who contributed 7 898 208 and 8 049 306 person years of observation, respectively. There were 24 350 incident diagnoses of osteoporotic fracture in women and 7934 in men, and 9302 incident diagnoses of hip fracture in women and 5424 in men.
Main outcome measures: First (incident) diagnosis of osteoporotic fracture (vertebral, distal radius, or hip) and incident hip fracture recorded in general practice records.
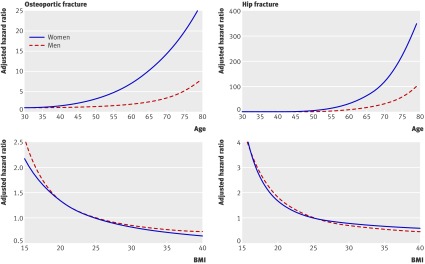
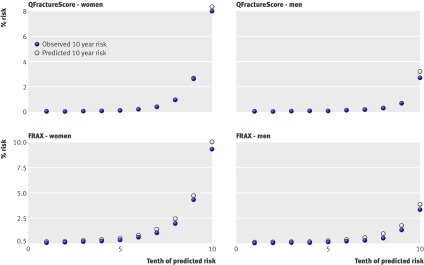
Results: Use of hormone replacement therapy (HRT), age, body mass index (BMI), smoking status, recorded alcohol use, parental history of osteoporosis, rheumatoid arthritis, cardiovascular disease, type 2 diabetes, asthma, tricyclic antidepressants, corticosteroids, history of falls, menopausal symptoms, chronic liver disease, gastrointestinal malabsorption, and other endocrine disorders were significantly and independently associated with risk of osteoporotic fracture in women. Some variables were significantly associated with risk of osteoporotic fracture but not with risk of hip fracture. The predictors for men for osteoporotic and hip fracture were age, BMI, smoking status, recorded alcohol use, rheumatoid arthritis, cardiovascular disease, type 2 diabetes, asthma, tricyclic antidepressants, corticosteroids, history of falls, and liver disease. The hip fracture algorithm had the best performance among men and women. It explained 63.94% of the variation in women and 63.19% of the variation in men. The D statistic values for discrimination were highest for hip fracture in women (2.73) and men (2.68) and were over twice the magnitude of the corresponding values for osteoporotic fracture. The ROC statistics for hip fracture were also high: 0.89 in women and 0.86 for men versus 0.79 and 0.69, respectively, for the osteoporotic fracture outcome. The algorithms were well calibrated with predicted risks closely matching observed risks. The QFractureScore for hip fracture also had good performance for discrimination and calibration compared with the FRAX (fracture risk assessment) algorithm.
Conclusions: These new algorithms can predict risk of fracture in primary care populations in the UK without laboratory measurements and are therefore suitable for use in both clinical settings and for self assessment (www.qfracture.org). QFractureScores could be used to identify patients at high risk of fracture who might benefit from interventions to reduce their risk.
Conflict of interest statement
Competing interests: JHC is codirector of QResearch, a not-for-profit organisation that is a joint partnership between the University of Nottingham and EMIS (leading supplier of IT for 60% of general practices in the UK). EMIS may implement the QFractureScore within its clinical system. JHC is also director of ClinRisk and CC is a consultant statistician for ClinRisk. ClinRisk produces software to ensure the reliable and updatable implementation of clinical risk algorithms within clinical computer systems to help improve patient care. This work and any views expressed within it are solely those of the co-authors and not of any affiliated bodies or organisations.
Figures
References
-
- National Institute for Health and Clinical Excellence. Systematic review of clinical effectiveness prepared for the guideline: “osteoporosis assessment of fracture risk and the prevention of osteoporotic fractures in individuals at high risk.” NICE, 2008.
-
- Dawson-Hughes B, Tosteson A, Melton L, Baim S, Favus M, Khosla S, et al. Implications of absolute fracture risk assessment for osteoporosis practice guidelines in the USA. Osteoporos Int 2008;19:449-58. - PubMed
-
- Kanis JA, McCloskey EV, Johansson H, Strom O, Borgstrom F, Oden A. Case finding for the management of osteoporosis with FRAX—assessment and intervention thresholds for the UK. Osteoporos Int 2008;19:1395-408. - PubMed
-
- National Osteoporosis Guideline Group. Guideline for the diagnosis and management of osteoporosis in postmenopausal men and women from the age of 50 in the UK. National Osteoporosis Guideline Group, 2008.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical