

Imaging of back pain in children
- PMID: 19926701
- PMCID: PMC7964168
- DOI: 10.3174/ajnr.A1832
Imaging of back pain in children
Abstract
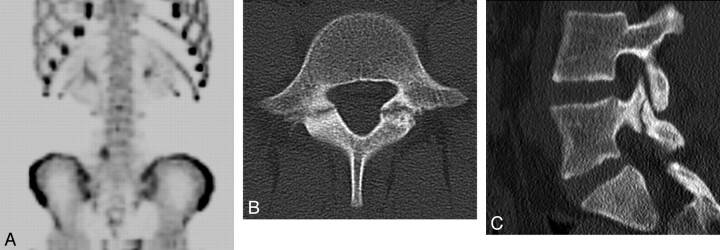
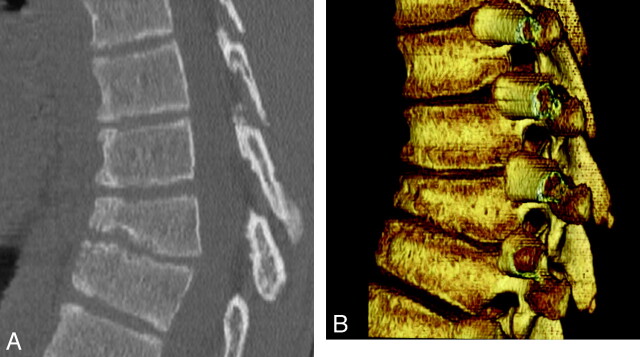
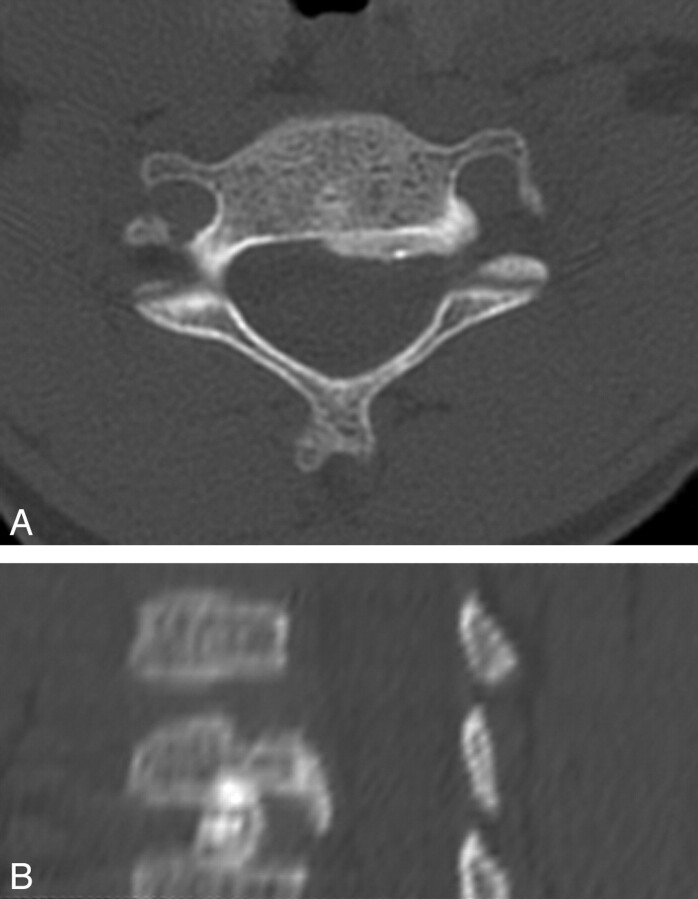
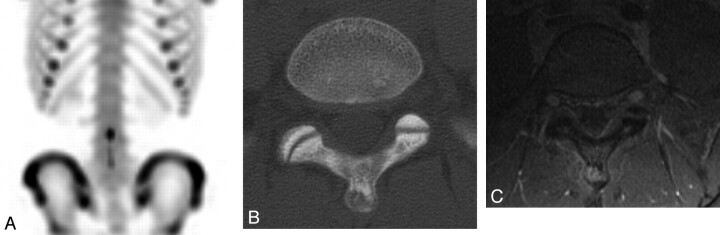
While back pain presents less frequently in children than in adults, it still poses a significant clinical challenge with respect to making a firm diagnosis and developing an effective treatment plan. When children have back pain and medical attention is sought, an underlying pathology is usually suspected. Pediatric patients are evaluated, first, with a complete clinical history and examination and, second, by an imaging work-up that is based on initial findings, including the child's age and size, signs and symptoms, and suspected etiology. This article describes 1) the epidemiology of back pain in children, 2) the imaging work-up used, and 3) the correlation of imaging findings with disease entities that may cause back pain in the pediatric patient. The list of diseases giving rise to back pain is not meant to be exhaustive but rather reflective of the most commonly identified pathologies and disorders among young children and adolescents, from athletic injuries to lethal cancers.
Figures







References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical