

High-resolution entrainment mapping of gastric pacing: a new analytical tool
- PMID: 19926815
- PMCID: PMC2822498
- DOI: 10.1152/ajpgi.00389.2009
High-resolution entrainment mapping of gastric pacing: a new analytical tool
Abstract
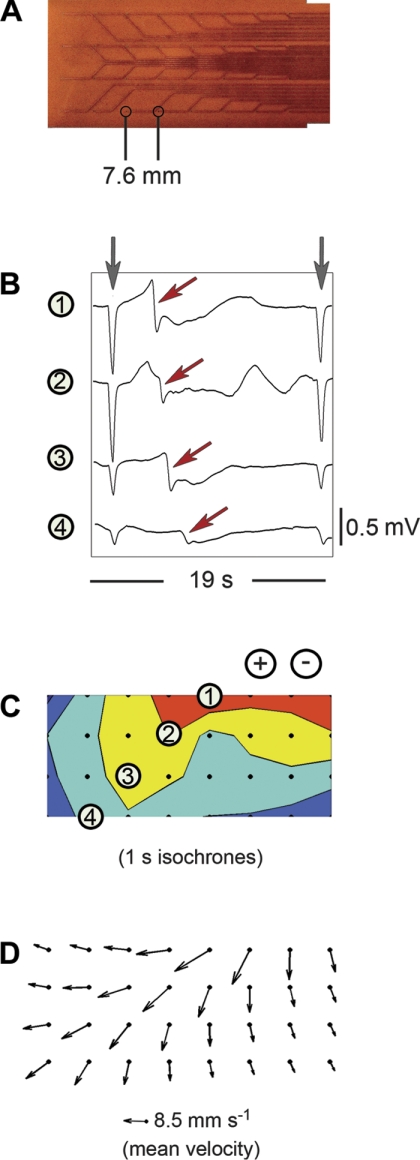
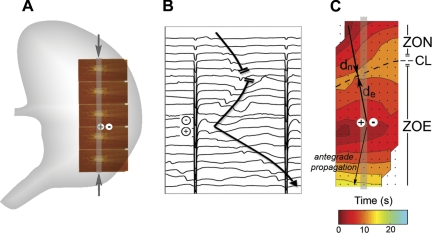
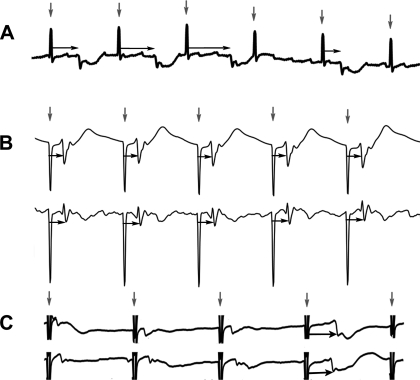
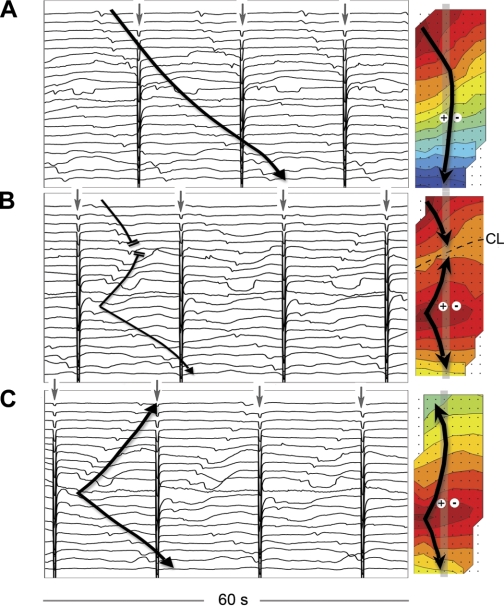
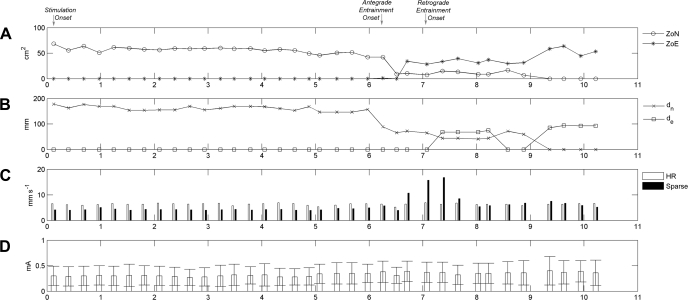
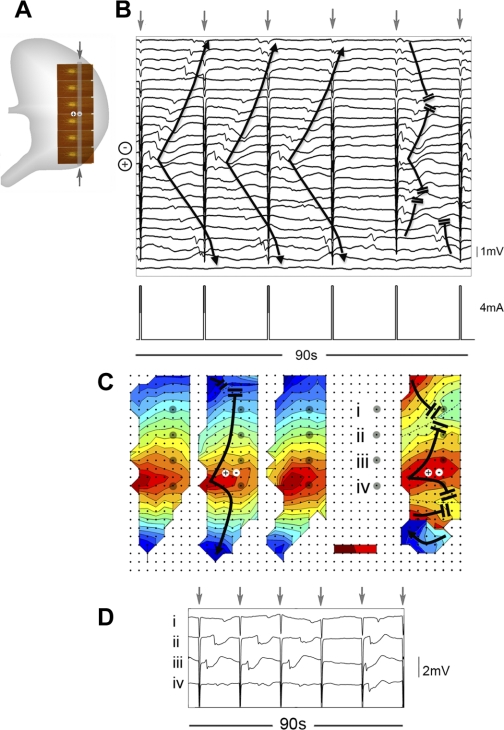
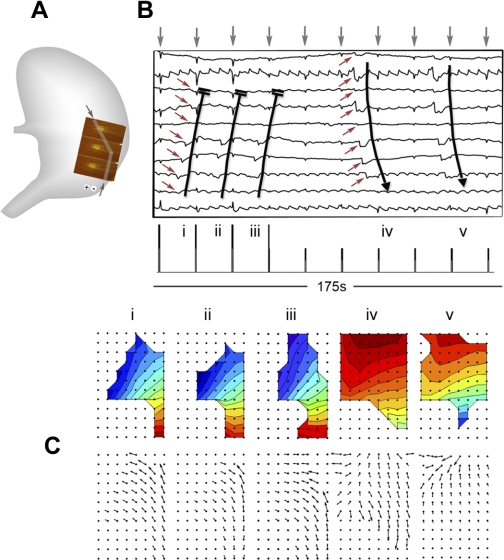
Gastric pacing has been investigated as a potential treatment for gastroparesis. New pacing protocols are required to improve symptom and motility outcomes; however, research progress has been constrained by a limited understanding of the effects of electrical stimulation on slow-wave activity. This study introduces high-resolution (HR) "entrainment mapping" for the analysis of gastric pacing and presents four demonstrations. Gastric pacing was initiated in a porcine model (typical amplitude 4 mA, pulse width 400 ms, period 17 s). Entrainment mapping was performed using flexible multielectrode arrays (</=192 electrodes; 92 cm(2)) and was analyzed using novel software methods. In the first demonstration, entrainment onset was quantified over successive waves in spatiotemporal detail. In the second demonstration, slow-wave velocity was accurately determined with HR field analysis, and paced propagation was found to be anisotropic (longitudinal 2.6 +/- 1.7 vs. circumferential 4.5 +/- 0.6 mm/s; P < 0.001). In the third demonstration, a dysrhythmic episode that occurred during pacing was mapped in HR, revealing an ectopic slow-wave focus and uncoupled propagations. In the fourth demonstration, differences were observed between paced and native slow-wave amplitudes (0.24 +/- 0.08 vs. 0.38 +/- 0.14 mV; P < 0.001), velocities (6.2 +/- 2.8 vs. 11.5 +/- 4.7 mm/s; P < 0.001), and activated areas (20.6 +/- 1.9 vs. 32.8 +/- 2.6 cm(2); P < 0.001). Entrainment mapping enables an accurate quantification of the effects of gastric pacing on slow-wave activity, offering an improved method to assess whether pacing protocols are likely to achieve physiologically and clinically useful outcomes.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources