

Ten-year detection rate of brain arteriovenous malformations in a large, multiethnic, defined population
- PMID: 19926839
- PMCID: PMC2847493
- DOI: 10.1161/STROKEAHA.109.566018
Ten-year detection rate of brain arteriovenous malformations in a large, multiethnic, defined population
Abstract
Background and purpose: To evaluate whether increased neuroimaging use is associated with increased brain arteriovenous malformation (BAVM) detection, we examined detection rates in the Kaiser Permanente Medical Care Program of northern California between 1995 and 2004.
Methods: We reviewed medical records, radiology reports, and administrative databases to identify BAVMs, intracranial aneurysms (IAs: subarachnoid hemorrhage [SAH] and unruptured aneurysms), and other vascular malformations (OVMs: dural fistulas, cavernous malformations, Vein of Galen malformations, and venous malformations). Poisson regression (with robust standard errors) was used to test for trend. Random-effects meta-analysis generated a pooled measure of BAVM detection rate from 6 studies.
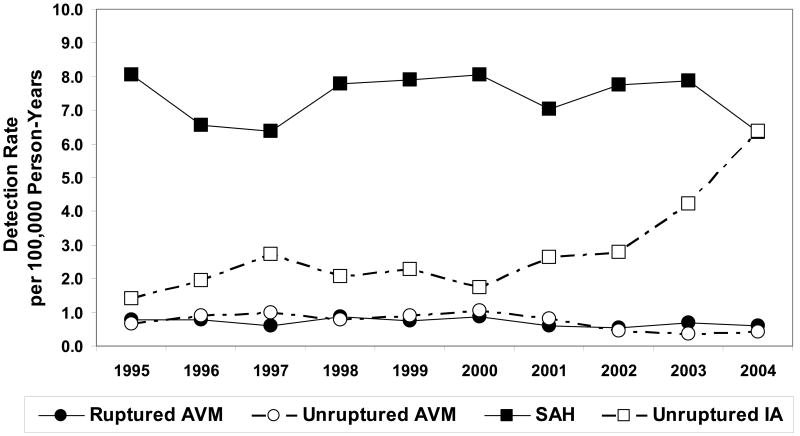
Results: We identified 401 BAVMs (197 ruptured, 204 unruptured), 570 OVMs, and 2892 IAs (2079 SAHs and 813 unruptured IAs). Detection rates per 100 000 person-years were 1.4 (95% CI, 1.3 to 1.6) for BAVMs, 2.0 (95% CI, 1.8 to 2.3) for OVMs, and 10.3 (95% CI, 9.9 to 10.7) for IAs. Neuroimaging utilization increased 12% per year during the time period (P<0.001). Overall, rates increased for IAs (P<0.001), remained stable for OVMs (P=0.858), and decreased for BAVMs (P=0.001). Detection rates increased 15% per year for unruptured IAs (P<0.001), with no change in SAHs (P=0.903). However, rates decreased 7% per year for unruptured BAVMs (P=0.016) and 3% per year for ruptured BAVMs (P=0.005). Meta-analysis yielded a pooled BAVM detection rate of 1.3 (95% CI, 1.2 to 1.4) per 100 000 person-years, without heterogeneity between studies (P=0.25).
Conclusions: Rates for BAVMs, OVMs, and IAs in this large, multiethnic population were similar to those in other series. During 1995 to 2004, a period of increasing neuroimaging utilization, we did not observe an increased rate of detection of unruptured BAVMs, despite increased detection of unruptured IAs.
Figures




References
-
- Al-Shahi R, Warlow C. A systematic review of the frequency and prognosis of arteriovenous malformations of the brain in adults. Brain. 2001;124:1900–1926. - PubMed
-
- Hofmeister C, Stapf C, Hartmann A, Sciacca RR, Mansmann U, terBrugge K, Lasjaunias P, Mohr JP, Mast H, Meisel J. Demographic, morphological, and clinical characteristics of 1289 patients with brain arteriovenous malformation. Stroke. 2000;31:1307–1310. - PubMed
-
- Choi JH, Mohr JP. Brain arteriovenous malformations in adults. Lancet Neurol. 2005;4:299–308. - PubMed
-
- Yamada S, Takagi Y, Nozaki K, Kikuta K, Hashimoto N. Risk factors for subsequent hemorrhage in patients with cerebral arteriovenous malformations. J Neurosurg. 2007;107:965–972. - PubMed
-
- Kim H, Sidney S, McCulloch CE, Poon KY, Singh V, Johnston SC, Ko NU, Achrol AS, Lawton MT, Higashida RT, Young WL. Racial/ethnic differences in longitudinal risk of intracranial hemorrhage in brain arteriovenous malformation patients. Stroke. 2007;38:2430–2437. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
