

A review on the molecular diagnostics of Lynch syndrome: a central role for the pathology laboratory
- PMID: 19929944
- PMCID: PMC3837620
- DOI: 10.1111/j.1582-4934.2009.00977.x
A review on the molecular diagnostics of Lynch syndrome: a central role for the pathology laboratory
Abstract
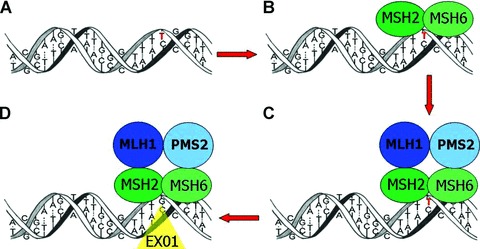
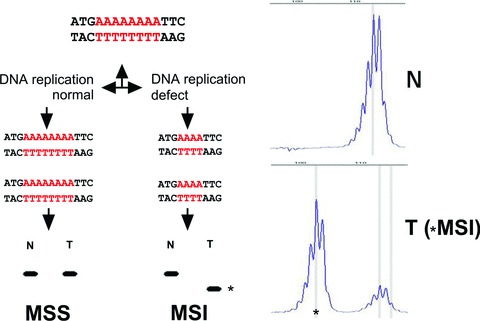
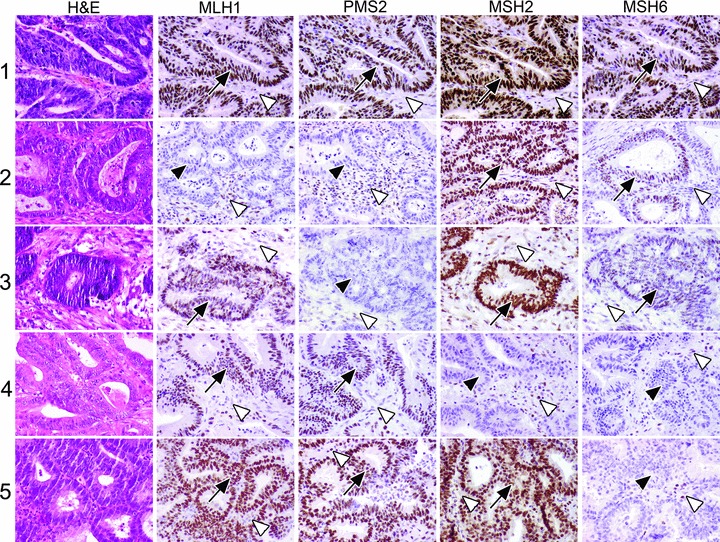
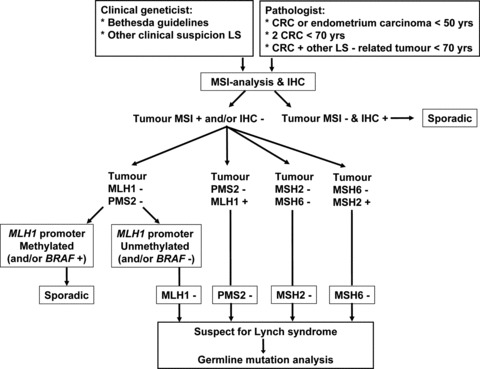
Lynch syndrome (LS) is caused by mutations in mismatch repair genes and is characterized by a high cumulative risk for the development of mainly colorectal carcinoma and endometrial carcinoma. Early detection of LS is important since surveillance can reduce morbidity and mortality. However, the diagnosis of LS is complicated by the absence of a pre-morbid phenotype and germline mutation analysis is expensive and time consuming. Therefore it is standard practice to precede germline mutation analysis by a molecular diagnostic work-up of tumours, guided by clinical and pathological criteria, to select patients for germline mutation analysis. In this review we address these molecular analyses, the central role for the pathologist in the selection of patients for germline diagnostics of LS, as well as the molecular basis of LS.
Figures
Similar articles
-
BRAF mutation analysis is a valid tool to implement in Lynch syndrome diagnosis in patients classified according to the Bethesda guidelines.Tumori. 2014 May-Jun;100(3):315-20. doi: 10.1700/1578.17214. Tumori. 2014. PMID: 25076244
-
Simplified identification of Lynch syndrome: a prospective, multicenter study.Dig Liver Dis. 2012 Jun;44(6):515-22. doi: 10.1016/j.dld.2011.12.020. Epub 2012 Apr 3. Dig Liver Dis. 2012. PMID: 22480969 Clinical Trial.
-
Yield of routine molecular analyses in colorectal cancer patients ≤70 years to detect underlying Lynch syndrome.J Pathol. 2012 Apr;226(5):764-74. doi: 10.1002/path.3963. Epub 2012 Jan 17. J Pathol. 2012. PMID: 22081473
-
[Colorectal Carcinoma with Suspected Lynch Syndrome: A Multidisciplinary Algorithm].Zentralbl Chir. 2015 Dec;140(6):591-9. doi: 10.1055/s-0034-1368480. Epub 2014 Nov 5. Zentralbl Chir. 2015. PMID: 25372301 Review. German.
-
[EPICOLON project: contribution to the knowledge of Lynch syndrome and other familial or hereditary colorectal cancer].Med Clin (Barc). 2007 Jan 20;128(2):55-60. doi: 10.1157/13097470. Med Clin (Barc). 2007. PMID: 17266903 Review. Spanish. No abstract available.
Cited by
-
Novel Implications in Molecular Diagnosis of Lynch Syndrome.Gastroenterol Res Pract. 2017;2017:2595098. doi: 10.1155/2017/2595098. Epub 2017 Jan 29. Gastroenterol Res Pract. 2017. PMID: 28250766 Free PMC article. Review.
-
Molecular classification of anaplastic oligodendroglioma using next-generation sequencing: a report of the prospective randomized EORTC Brain Tumor Group 26951 phase III trial.Neuro Oncol. 2016 Mar;18(3):388-400. doi: 10.1093/neuonc/nov182. Epub 2015 Sep 9. Neuro Oncol. 2016. PMID: 26354927 Free PMC article. Clinical Trial.
-
Comparison of screening strategies for Lynch syndrome in patients with newly diagnosed endometrial cancer: a prospective cohort study in China.Cancer Commun (Lond). 2019 Jul 15;39(1):42. doi: 10.1186/s40880-019-0388-2. Cancer Commun (Lond). 2019. PMID: 31307542 Free PMC article.
-
Lynch Syndrome: Its Impact on Urothelial Carcinoma.Int J Mol Sci. 2021 Jan 7;22(2):531. doi: 10.3390/ijms22020531. Int J Mol Sci. 2021. PMID: 33430305 Free PMC article. Review.
-
DNA mismatch repair and infertility.Curr Opin Urol. 2010 Nov;20(6):525-32. doi: 10.1097/MOU.0b013e32833f1c21. Curr Opin Urol. 2010. PMID: 20852424 Free PMC article. Review.
References
-
- Boyle P, Ferlay J. Cancer incidence and mortality in Europe, 2004. Ann Oncol. 2005;16:481–8. - PubMed
-
- Aaltonen LA, Salovaara R, Kristo P, et al. Incidence of hereditary nonpolyposis colorectal cancer and the feasibility of molecular screening for the disease. N Engl J Med. 1998;338:1481–7. - PubMed
-
- Hampel H, Frankel W, Panescu J, et al. Screening for Lynch syndrome (hereditary nonpolyposis colorectal cancer) among endometrial cancer patients. Cancer Res. 2006;66:7810–7. - PubMed
-
- Lynch HT, Smyrk TC, Watson P, et al. Genetics, natural history, tumor spectrum, and pathology of hereditary nonpolyposis colorectal cancer: an updated review. Gastroenterology. 1993;104:1535–49. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
