

Assessing Heterogeneity of Treatment Effects: Are Authors Misinterpreting Their Results?
- PMID: 19929962
- PMCID: PMC2813449
- DOI: 10.1111/j.1475-6773.2009.01064.x
Assessing Heterogeneity of Treatment Effects: Are Authors Misinterpreting Their Results?
Abstract
Objective: To determine whether investigations of heterogeneity of treatment effects (HTE) in randomized-controlled trials (RCTs) are prespecified and whether authors' interpretations of their analyses are consistent with the objective evidence.
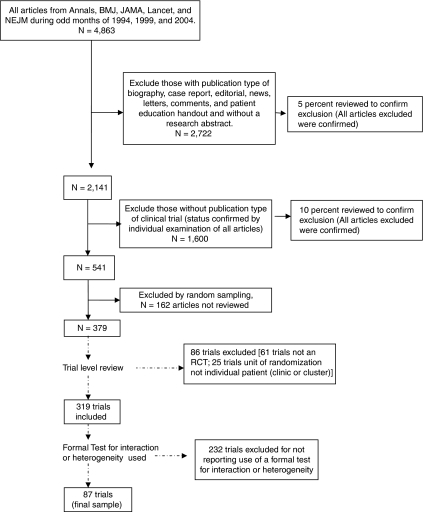
Data sources/study setting: Trials published in Annals of Internal Medicine, British Medical Journal, Journal of the American Medical Association, Lancet, and New England Journal of Medicine in 1994, 1999, and 2004.
Study design: We reviewed 87 RCTs that reported formal tests for statistical interaction or heterogeneity (HTE analyses), derived from a probability sample of 541 articles.
Data collection/extraction: We recorded reasons for performing HTE analysis; an objective classification of evidence for HTE (termed "clinicostatistical divergence" [CSD]); and authors' interpretations of findings. Authors' interpretations, compared with CSD, were coded as understated, overstated, or adequately stated.
Principle findings: Fifty-three RCTs (61 percent) claimed prespecified covariates for HTE analyses. Trials showed strong (6), moderate (11), weak (25), or negligible (16) evidence for CSD (29 could not be classified due to inadequate information). Authors stated that evidence for HTE was sufficient to support differential treatment in subgroups (10); warranted more research (31); was absent (21); or provided no interpretation (25). HTE was overstated in 22 trials, adequately stated in 57 trials, and understated in 8 trials.
Conclusions: Inconsistencies in performance and reporting may limit the potential of HTE analysis as a tool for identifying HTE and individualizing care in diverse populations. Recommendations for future studies on the reporting and interpretation of HTE analyses are provided.
Figures
References
-
- Altman DG, Schulz KF, Moher D, Egger M, Davidoff F, Elbourne D, Getzche PC, Lang T. The Revised CONSORT Statement for Reporting Trials: Explanation and Elaboration. Annals of Internal Medicine. 2001;134(8):663–94. - PubMed
-
- Assmann SF, Pocock SJ, Enos LE, Kasten LE. Subgroup Analysis and Other (Mis)uses of Baseline Data in Clinical Trials. Lancet. 2000;355:1064–9. - PubMed
-
- Baird KL. The New NIH and FDA Medical Research Policies: Targeting Gender, Promoting Justice. Journal of Health Politics, Policy, and Law. 1999;24(3):531–65. - PubMed
-
- Brookes ST, Whitely E, Egger M, Smith GD, Mulheran PA, Peters TJ. Subgroup Analyses in Randomized Trials: Risks of Subgroup-Specific Analyses; Power and Sample Size for the Interaction Test. Journal of Clinical Epidemiology. 2004;57:229–36. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
