

Advances in the management and understanding of autoimmune lymphoproliferative syndrome (ALPS)
- PMID: 19930184
- PMCID: PMC2929682
- DOI: 10.1111/j.1365-2141.2009.07991.x
Advances in the management and understanding of autoimmune lymphoproliferative syndrome (ALPS)
Abstract
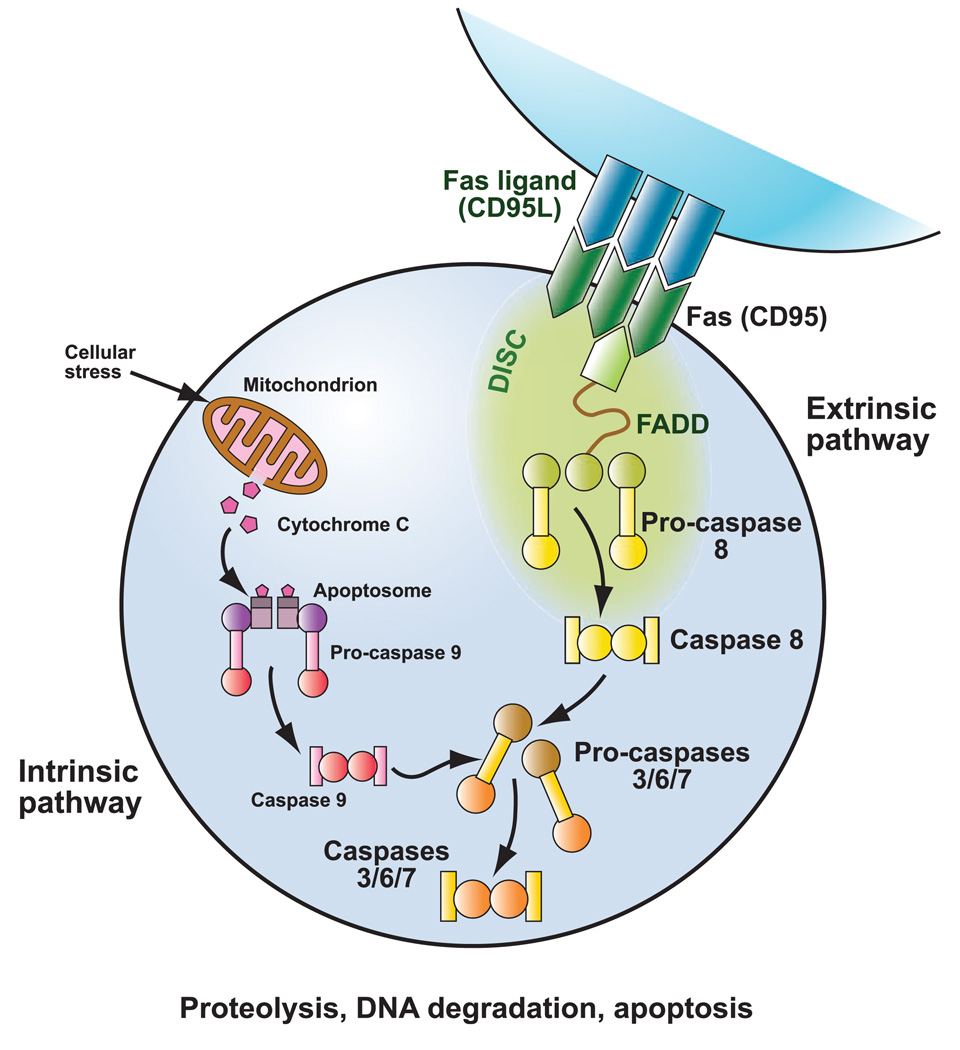
Autoimmune lymphoproliferative syndrome (ALPS) is a disorder of T cell dysregulation caused by defective Fas-mediated apoptosis. Patients with ALPS can develop a myriad of clinical manifestations including lymphadenopathy, hepatosplenomegaly, autoimmunity and increased rates of malignancy. ALPS may be more common that originally thought, and testing for ALPS should be considered in patients with unexplained lymphadenopathy, hepatosplenomegaly, and/or autoimmunity. As the pathophysiology of ALPS is better characterized, a number of targeted therapies are in preclinical development and clinical trials with promising early results. This review describes the clinical and laboratory manifestations found in ALPS patients, as well as the molecular basis for the disease and new advances in treatment.
Figures
Similar articles
-
Updated Understanding of Autoimmune Lymphoproliferative Syndrome (ALPS).Clin Rev Allergy Immunol. 2016 Feb;50(1):55-63. doi: 10.1007/s12016-015-8466-y. Clin Rev Allergy Immunol. 2016. PMID: 25663566 Review.
-
Advances in autoimmune lymphoproliferative syndromes.Eur J Haematol. 2011 Jul;87(1):1-9. doi: 10.1111/j.1600-0609.2011.01617.x. Eur J Haematol. 2011. PMID: 21447005 Review.
-
New advances in the diagnosis and treatment of autoimmune lymphoproliferative syndrome.Curr Opin Pediatr. 2012 Feb;24(1):1-8. doi: 10.1097/MOP.0b013e32834ea739. Curr Opin Pediatr. 2012. PMID: 22157362 Free PMC article. Review.
-
Autoimmune lymphoproliferative syndrome: an update and review of the literature.Curr Allergy Asthma Rep. 2014 Sep;14(9):462. doi: 10.1007/s11882-014-0462-4. Curr Allergy Asthma Rep. 2014. PMID: 25086580 Free PMC article. Review.
-
Autoimmune Lymphoproliferative Syndrome in Children with Nonmalignant Organomegaly, Chronic Immune Cytopenia, and Newly Diagnosed Lymphoma.Turk J Haematol. 2021 Jun 1;38(2):145-150. doi: 10.4274/tjh.galenos.2020.2020.0618. Epub 2020 Dec 30. Turk J Haematol. 2021. PMID: 33375216 Free PMC article.
Cited by
-
Updated Understanding of Autoimmune Lymphoproliferative Syndrome (ALPS).Clin Rev Allergy Immunol. 2016 Feb;50(1):55-63. doi: 10.1007/s12016-015-8466-y. Clin Rev Allergy Immunol. 2016. PMID: 25663566 Review.
-
Genes and Microbiota Interaction in Monogenic Autoimmune Disorders.Biomedicines. 2023 Apr 8;11(4):1127. doi: 10.3390/biomedicines11041127. Biomedicines. 2023. PMID: 37189745 Free PMC article. Review.
-
Late-Onset Autoimmune Lymphoproliferative Syndrome in a Costa Rican Woman.Cureus. 2023 Dec 9;15(12):e50226. doi: 10.7759/cureus.50226. eCollection 2023 Dec. Cureus. 2023. PMID: 38077666 Free PMC article.
-
Clues to immune tolerance: the monogenic autoimmune syndromes.Ann N Y Acad Sci. 2010 Dec;1214:138-55. doi: 10.1111/j.1749-6632.2010.05818.x. Epub 2010 Oct 22. Ann N Y Acad Sci. 2010. PMID: 20969580 Free PMC article. Review.
-
Genetic Characterization of Short Stature Patients With Overlapping Features of Growth Hormone Insensitivity Syndromes.J Clin Endocrinol Metab. 2021 Oct 21;106(11):e4716-e4733. doi: 10.1210/clinem/dgab437. J Clin Endocrinol Metab. 2021. PMID: 34136918 Free PMC article.
References
-
- Abdel-Karim IA, Giles FJ. Mammalian target of rapamycin as a target in hematological malignancies. Current Problems in Cancer. 2008;32:161–177. - PubMed
-
- Auricchio L, Vitiello L, Adriani M, Ferri P, Chiocchetti A, Pettinato G, Racioppi L, Maiuri L, Dianzani U, Pignata C. Cutaneous manifestations as presenting sign of autoimmune lymphoproliferative syndrome in childhood. Dermatology. 2005;210:336–340. - PubMed
-
- Bakker NA, van Imhoff GW, Verschuuren EA, van Son WJ. Presentation and early detection of post-transplant lymphoproliferative disorder after solid organ transplantation. Transplant International. 2007;20:207–218. - PubMed
-
- Bleesing JJ. Autoimmune lymphoproliferative syndrome: a genetic disorder of abnormal lymphocyte apoptosis. Immunology and Allergy Clinics of North America. 2002;22:339–349. - PubMed
-
- Bleesing JJ. Autoimmune lymphoproliferative syndrome (ALPS) Current Pharmaceutical Design. 2003;9:265–278. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
