

Evaluating overall survival and competing risks of death in patients with localized renal cell carcinoma using a comprehensive nomogram
- PMID: 19933918
- PMCID: PMC2815719
- DOI: 10.1200/JCO.2009.22.4816
Evaluating overall survival and competing risks of death in patients with localized renal cell carcinoma using a comprehensive nomogram
Abstract
Purpose: Many patients with localized node-negative renal cell carcinoma (RCC) are elderly with competing comorbidities. Their overall survival benefit after surgical treatment is unknown. We reviewed cases in the Surveillance, Epidemiology, and End Results (SEER) database to evaluate the impact of kidney cancer versus competing causes of death in patients with localized RCC and develop a comprehensive nomogram to quantitate survival differences.
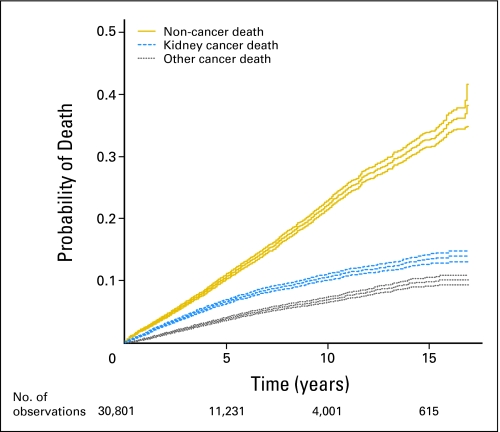
Methods: We identified individuals with localized, surgically treated clear-cell, papillary, or chromophobe RCC in SEER (1988 through 2003). We used Fine and Gray competing risks proportional hazards regressions to predict 5-year probabilities of three competing mortality outcomes: kidney cancer death, other cancer death, and noncancer death.
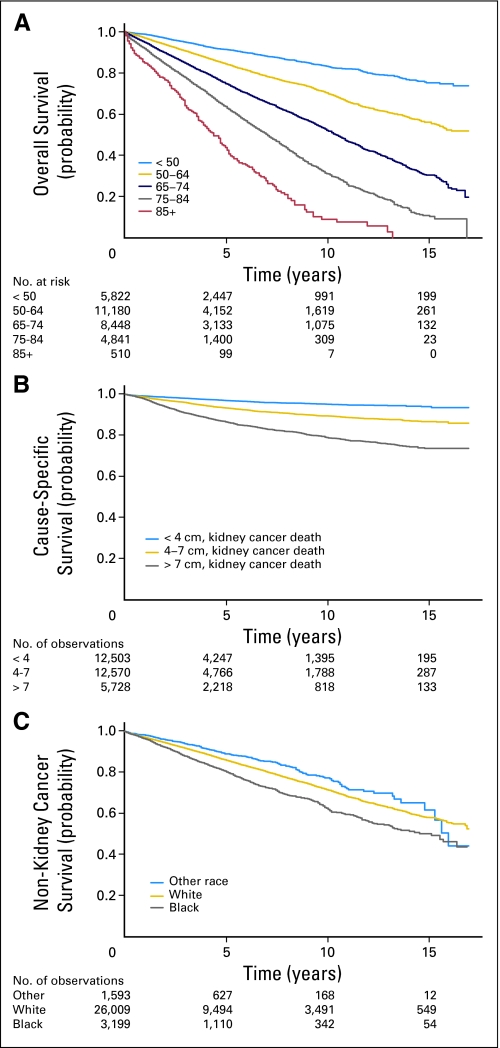
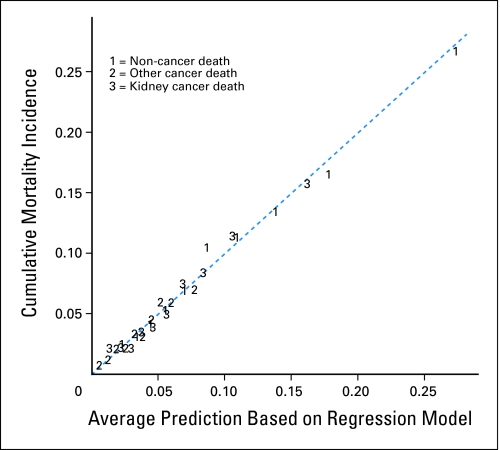
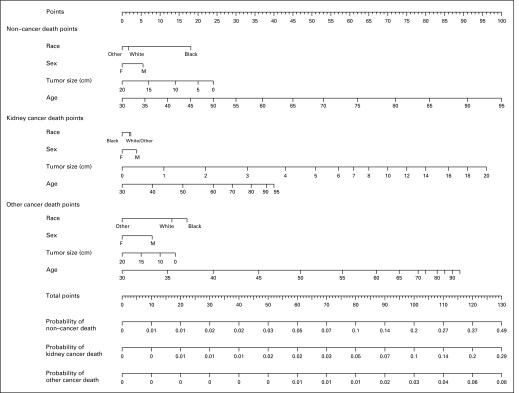
Results: We identified 30,801 cases of localized RCC (median age, 62 years; median tumor size, 4.5 cm). Five-year probabilities of kidney cancer death, other cancer death, and noncancer death were 4%, 7%, and 11%, respectively. Age was strongly predictive of mortality and most predictive of nonkidney cancer deaths (P < .001). Increasing tumor size was related to death from RCC and inversely related to noncancer deaths (P < .001). Racial differences in outcomes were most pronounced for nonkidney cancer deaths (P < .001). Men were more likely to die than women from all causes (P < .002). This nomogram integrates commonly available factors into a useful tool for comparing competing risks of death.
Conclusion: Management of localized RCC must consider competing causes of mortality, particularly in elderly populations. Effective decision making requires treatment trade-off calculations. We present a tool to quantitate competing causes of mortality in patients with localized RCC.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Population-based external validation of a competing-risks nomogram for patients with localized renal cell carcinoma.J Clin Oncol. 2010 Jun 20;28(18):e299-300; author reply e301. doi: 10.1200/JCO.2009.27.6345. Epub 2010 May 17. J Clin Oncol. 2010. PMID: 20479402 No abstract available.
-
Importance of comorbidity in competing risks analysis in patients with localized renal cell carcinoma.J Clin Oncol. 2010 Jun 20;28(18):e298; author reply e301. doi: 10.1200/JCO.2009.27.3987. Epub 2010 May 17. J Clin Oncol. 2010. PMID: 20479414 No abstract available.
References
-
- Chawla SN, Crispen PL, Hanlon AL, et al. The natural history of observed enhancing renal masses: Meta-analysis and review of the world literature. J Urol. 2006;175:425–431. - PubMed
-
- Hollingsworth JM, Miller DC, Daignault S, et al. Rising incidence of small renal masses: A need to reassess treatment effect. J Natl Cancer Inst. 2006;98:1331–1334. - PubMed
-
- Parsons JK, Schoenberg MS, Carter HB. Incidental renal tumors: Casting doubt on the efficacy of early intervention. Urology. 2001;57:1013–1015. - PubMed
-
- Kunkle DA, Egleston BL, Uzzo RG. Excise, ablate or observe: The small renal mass dilemma—A meta-analysis and review. J Urol. 2008;179:1227–1233. - PubMed
-
- Lane BR, Babineau D, Kattan MW, et al. A preoperative prognostic nomogram for solid enhancing renal tumors 7 cm or less amenable to partial nephrectomy. J Urol. 2007;178:429–434. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
