

Physician and pharmacist collaboration to improve blood pressure control
- PMID: 19933962
- PMCID: PMC2882170
- DOI: 10.1001/archinternmed.2009.358
Physician and pharmacist collaboration to improve blood pressure control
Abstract
Background: Studies have demonstrated that blood pressure (BP) control can be improved when clinical pharmacists assist with patient management. The objective of this study was to evaluate if a physician and pharmacist collaborative model in community-based medical offices could improve BP control.
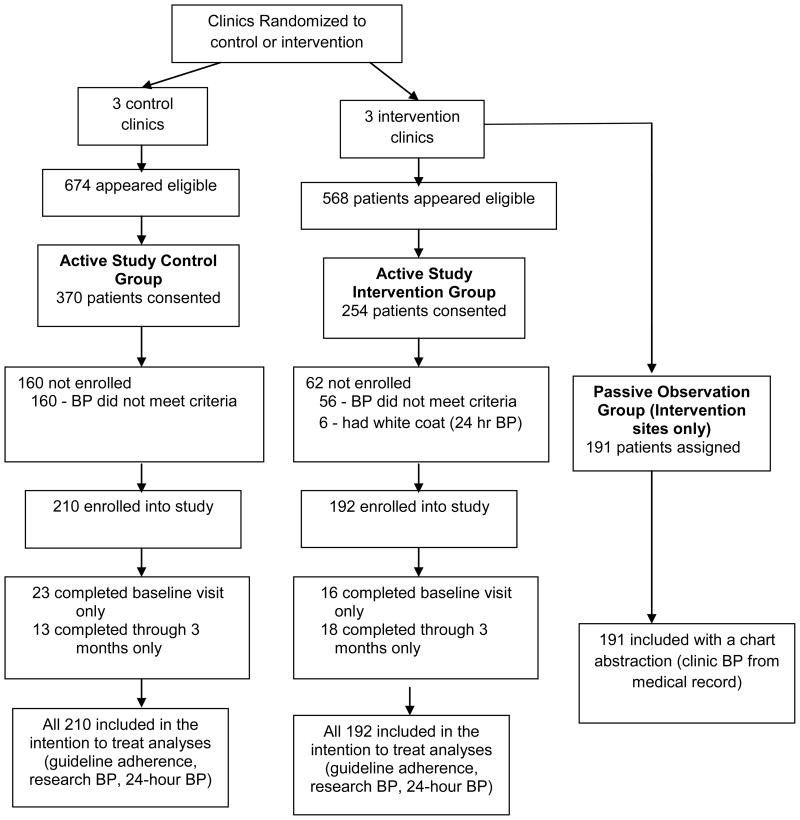
Methods: This was a prospective, cluster randomized, controlled clinical trial with clinics randomized to a control group (n = 3) or to an intervention group (n = 3). The study enrolled 402 patients (mean age, 58.3 years) with uncontrolled hypertension. Clinical pharmacists made drug therapy recommendations to physicians based on national guidelines. Research nurses performed BP measurements and 24-hour BP monitoring.
Results: The mean (SD) guideline adherence scores increased from 49.4 (19.3) at baseline to 53.4 (18.1) at 6 months (8.1% increase) in the control group and from 40.4 (22.6) at baseline to 62.8 (13.5) at 6 months (55.4% increase) in the intervention group (P = .09 for adjusted between-group comparison). The mean BP decreased 6.8/4.5 mm Hg in the control group and 20.7/9.7 mm Hg in the intervention group (P < .05 for between-group systolic BP comparison). The adjusted difference in systolic BP was -12.0 (95% confidence interval [CI], -24.0 to 0.0) mm Hg, while the adjusted difference in diastolic BP was -1.8 (95% CI, -11.9 to 8.3) mm Hg. The 24-hour BP levels showed similar effect sizes. Blood pressure was controlled in 29.9% of patients in the control group and in 63.9% of patients in the intervention group (adjusted odds ratio, 3.2; 95% CI, 2.0-5.1; P < .001).
Conclusions: A physician and pharmacist collaborative intervention achieved significantly better mean BP and overall BP control rates compared with a control group. Additional research should be conducted to evaluate efficient strategies to implement team-based chronic disease management.
Trial registration: clinicaltrials.gov Identifier: NCT00201019.
Figures
Comment in
-
Home is where the health is: advancing team-based care in chronic disease management.Arch Intern Med. 2009 Nov 23;169(21):1945-8. doi: 10.1001/archinternmed.2009.428. Arch Intern Med. 2009. PMID: 19933953 No abstract available.
-
Case management to reduce risk of cardiovascular disease in a county health care system.Arch Intern Med. 2009 Nov 23;169(21):1988-95. doi: 10.1001/archinternmed.2009.381. Arch Intern Med. 2009. PMID: 19933961 Free PMC article. Clinical Trial.
-
Impact of a pharmacist-facilitated hospital discharge program: a quasi-experimental study.Arch Intern Med. 2009 Nov 23;169(21):2003-10. doi: 10.1001/archinternmed.2009.398. Arch Intern Med. 2009. PMID: 19933963
References
-
- Carter BL, Malone DC, Ellis SL, Dombrowski RC. Antihypertensive Drug Utilization in Hypertensive Veterans With Complex Medication Profiles. J Clin Hypertens. 2000;2:172–180. - PubMed
-
- Naiman DJ, Barker LR. Adherence to the JNC VI guidelines for the treatment of hypertension in the resident clinic. Maryland Medical Journal. 1999;48:307–311. - PubMed
-
- Nelson CR, Knapp DA. Trends in antihypertensive drug therapy of ambulatory patients by US office-based physicians. Hypertension. 2000;36:600–603. - PubMed
