

Donor treatment with a PHD-inhibitor activating HIFs prevents graft injury and prolongs survival in an allogenic kidney transplant model
- PMID: 19934037
- PMCID: PMC2795511
- DOI: 10.1073/pnas.0903978106
Donor treatment with a PHD-inhibitor activating HIFs prevents graft injury and prolongs survival in an allogenic kidney transplant model
Abstract
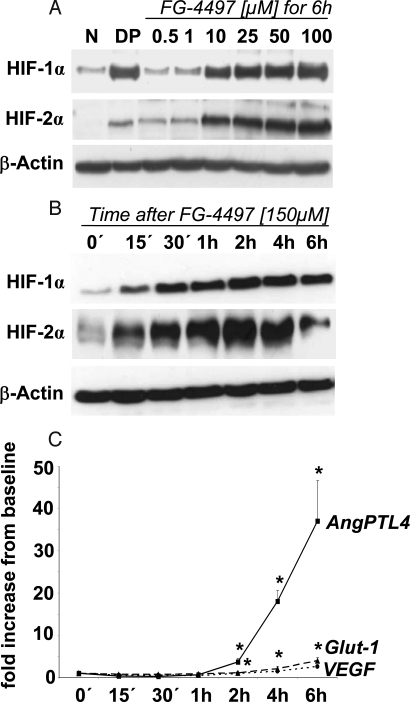
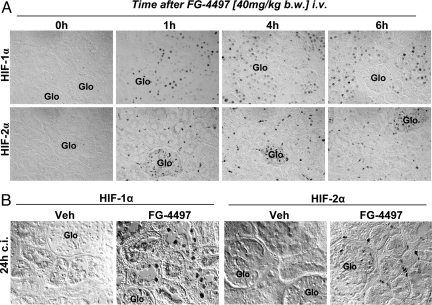
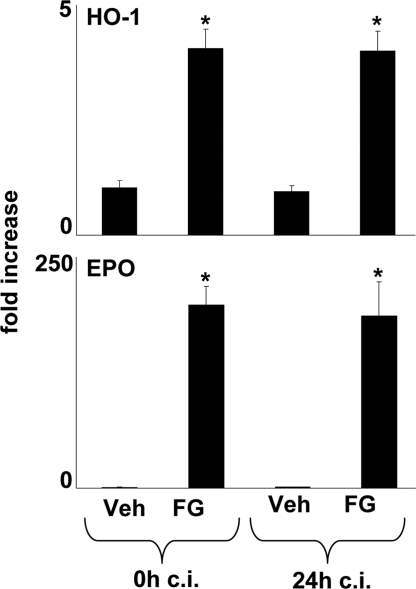
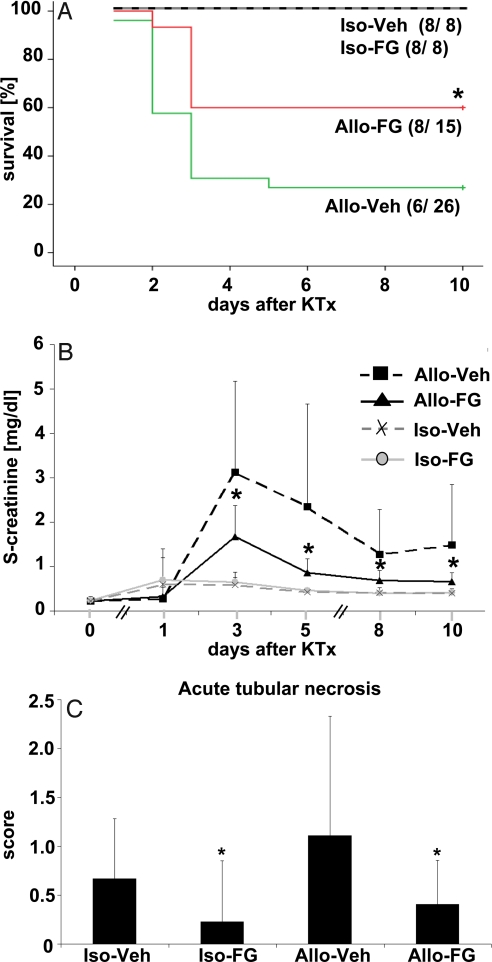
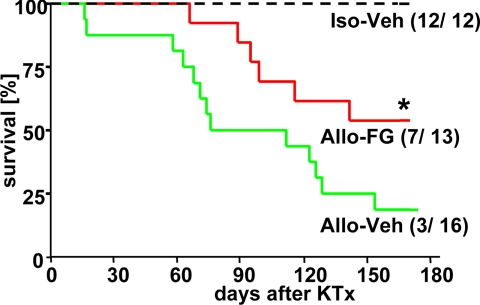
Long-term survival of renal allografts depends on the chronic immune response and is probably influenced by the initial injury caused by ischemia and reperfusion. Hypoxia-inducible transcription factors (HIFs) are essential for adaptation to low oxygen. Normoxic inactivation of HIFs is regulated by oxygen-dependent hydroxylation of specific prolyl-residues by prolyl-hydroxylases (PHDs). Pharmacological inhibition of PHDs results in HIF accumulation with subsequent activation of tissue-protective genes. We examined the effect of donor treatment with a specific PHD inhibitor (FG-4497) on graft function in the Fisher-Lewis rat model of allogenic kidney transplantation (KTx). Orthotopic transplantation of the left donor kidney was performed after 24 h of cold storage. The right kidney was removed at the time of KTx (acute model) or at day 10 (chronic model). Donor animals received a single dose of FG-4497 (40 mg/kg i.v.) or vehicle 6 h before donor nephrectomy. Recipients were followed up for 10 days (acute model) or 24 weeks (chronic model). Donor preconditioning with FG-4497 resulted in HIF accumulation and induction of HIF target genes, which persisted beyond cold storage. It reduced acute renal injury (serum creatinine at day 10: 0.66 +/- 0.20 vs. 1.49 +/- 1.36 mg/dL; P < 0.05) and early mortality in the acute model and improved long-term survival of recipient animals in the chronic model (mortality at 24 weeks: 3 of 16 vs. 7 of 13 vehicle-treated animals; P < 0.05). In conclusion, pretreatment of organ donors with FG-4497 improves short- and long-term outcomes after allogenic KTx. Inhibition of PHDs appears to be an attractive strategy for organ preservation that deserves clinical evaluation.
Conflict of interest statement
Conflict of interest statement: S.K., M.A., and L.F. are employees of FibroGen.
Figures
Similar articles
-
Reduction of obliterative bronchiolitis (OB) by prolyl-hydroxylase-inhibitors activating hypoxia-inducible transcription factors in an experimental mouse model.Transpl Immunol. 2016 Nov;39:66-73. doi: 10.1016/j.trim.2016.08.007. Epub 2016 Aug 30. Transpl Immunol. 2016. PMID: 27590486
-
Hydrogen Sulfide Treatment Mitigates Renal Allograft Ischemia-Reperfusion Injury during Cold Storage and Improves Early Transplant Kidney Function and Survival Following Allogeneic Renal Transplantation.J Urol. 2015 Dec;194(6):1806-15. doi: 10.1016/j.juro.2015.07.096. Epub 2015 Aug 1. J Urol. 2015. PMID: 26239336
-
The protective effect of prolyl-hydroxylase inhibition against renal ischaemia requires application prior to ischaemia but is superior to EPO treatment.Nephrol Dial Transplant. 2012 Mar;27(3):929-36. doi: 10.1093/ndt/gfr379. Epub 2011 Jul 8. Nephrol Dial Transplant. 2012. PMID: 21742784
-
HIF-prolyl hydroxylases and cardiovascular diseases.Toxicol Mech Methods. 2012 Jun;22(5):347-58. doi: 10.3109/15376516.2012.673088. Toxicol Mech Methods. 2012. PMID: 22424133 Review.
-
Protein Hydroxylation by Hypoxia-Inducible Factor (HIF) Hydroxylases: Unique or Ubiquitous?Cells. 2019 Apr 26;8(5):384. doi: 10.3390/cells8050384. Cells. 2019. PMID: 31035491 Free PMC article. Review.
Cited by
-
Roxadustat for Patients with Posttransplant Anemia: A Narrative Review.Kidney Dis (Basel). 2023 Nov 10;10(1):32-38. doi: 10.1159/000535071. eCollection 2024 Feb. Kidney Dis (Basel). 2023. PMID: 38322628 Free PMC article. Review.
-
Molecular oxygen sensing: implications for visceral surgery.Langenbecks Arch Surg. 2012 Apr;397(4):603-10. doi: 10.1007/s00423-012-0930-z. Epub 2012 Mar 7. Langenbecks Arch Surg. 2012. PMID: 22395314 Review.
-
Hypoxia-inducible factors in physiology and medicine.Cell. 2012 Feb 3;148(3):399-408. doi: 10.1016/j.cell.2012.01.021. Cell. 2012. PMID: 22304911 Free PMC article. Review.
-
William Kaelin, Peter Ratcliffe, and Gregg Semenza receive the 2016 Albert Lasker Basic Medical Research Award.J Clin Invest. 2016 Oct 3;126(10):3628-3638. doi: 10.1172/JCI90055. Epub 2016 Sep 13. J Clin Invest. 2016. PMID: 27620538 Free PMC article. No abstract available.
-
Early biomarkers of nephrotoxicity associated with the use of anti-VEGF drugs.Biomed Rep. 2022 Jun;16(6):46. doi: 10.3892/br.2022.1529. Epub 2022 Apr 7. Biomed Rep. 2022. PMID: 35620307 Free PMC article.
References
-
- Wolfe RA, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. 1999;341:1725–1730. - PubMed
-
- Meier-Kriesche HU, Schold JD, Kaplan B. Long-term renal allograft survival: Have we made significant progress or is it time to rethink our analytic and therapeutic strategies? Am J Transplant. 2004;4:1289–1295. - PubMed
-
- Vadivel N, Tullius SG, Chandraker A. Chronic allograft nephropathy. Semin Nephrol. 2007;27(4):414–429. - PubMed
-
- Kaplan B. Overcoming barriers to long-term graft survival. Am J Kidney Dis. 2006;47(4) suppl. 2:S52–S64. - PubMed
-
- Baid-Agrawal S, Frei UA. Living donor renal transplantation: Recent developments and perspectives. Nat Clin Pract Nephrol. 2007;3:31–41. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
