

Antiretroviral treatment changes in adults from Côte d'Ivoire: the roles of tuberculosis and pregnancy
- PMID: 19935382
- PMCID: PMC3936254
- DOI: 10.1097/QAD.0b013e32832ec1c3
Antiretroviral treatment changes in adults from Côte d'Ivoire: the roles of tuberculosis and pregnancy
Abstract
Objective: To determine the rates and causes of first antiretroviral treatment changes in HIV-infected adults in Côte d'Ivoire.
Methods: We evaluated adults who initiated antiretroviral treatment in an outpatient clinic in Abidjan. We recorded baseline and follow-up data, including drug prescriptions and reasons for changing to alternative first-line regimens (drug substitution for any reason but failure) or second-line regimens (switch for failure).
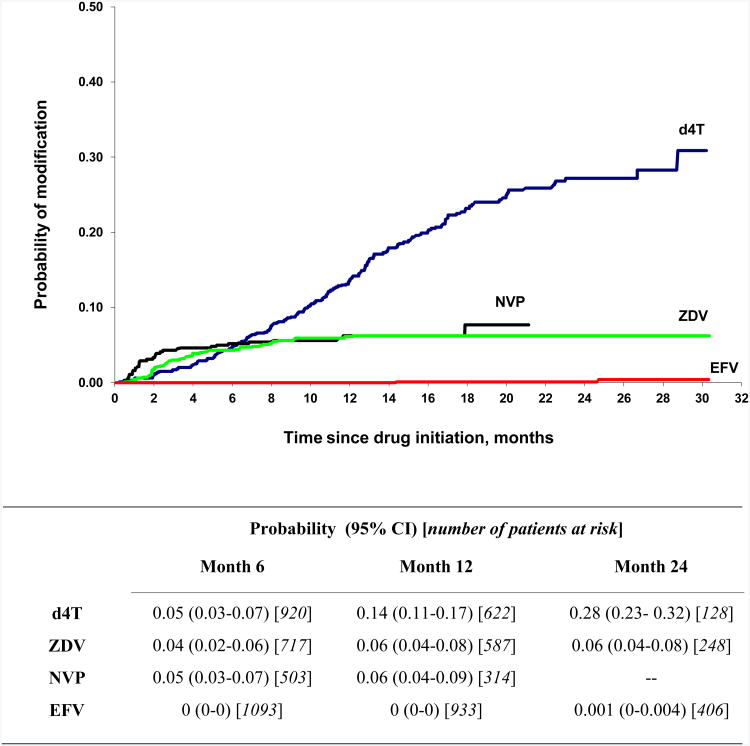
Results: Two thousand and twelve HIV-infected adults (73% women) initiated antiretroviral treatment. At baseline, 9% of all patients were on treatment for tuberculosis and 3% of women were pregnant. First-line antiretroviral treatment consisted of two nucleoside reverse transcriptase inhibitors (58% stavudine-lamivudine, 42% zidovudine-lamivudine) and efavirenz (63%), nevirapine (32%) or indinavir (5%). Median follow-up time was 16.9 months. During this time, 205 (10%) patients died and 261 (13%) were lost to follow-up. Overall, the rate of treatment modifications was 20.7/100 patient-years. The most common modifications were drug substitutions for intolerance (12.4/100 patient-years), pregnancy (4.5/100 patient-years) and tuberculosis (2.5/100 patient-years). The rates of intolerance-related substitutions were 17.9/100 patient-years for stavudine, 6.3/100 patient-years for nevirapine, 3.9/100 patient-years for zidovudine and 0.1/100 patient-years for efavirenz. Twenty percent of efavirenz substitutions resulted from pregnancy and 18% of nevirapine substitutions were related to tuberculosis treatment.
Conclusion: During the first months following antiretroviral treatment initiation, a third of all treatment changes occurred for reasons other than intolerance to the drug or treatment failure. In Africa, drug forecasting is crucial to ensuring the success of HIV treatment programmes. Drugs that do not require interruptions during pregnancy or tuberculosis treatment should be made more readily available as first-line drugs in sub-Saharan Africa.
Conflict of interest statement
Figures
Comment in
-
The importance of descriptive epidemiology from the developing world.AIDS. 2010 Jan 2;24(1):101-2. doi: 10.1097/QAD.0b013e328331e173. AIDS. 2010. PMID: 19734773 No abstract available.
References
-
- UNAIDS, WHO. AIDS epidemic update: Sub-Saharan Africa regional summary. 2007 http://data.unaids.org/pub/Report/2008/jc1526_epibriefs_ssafrica_en.pdf.
-
- WHO, UNAIDS, UNICEF. Towards universal access: scaling up priority HIV/AIDS interventions in the health sector: progress Report, 2008. http://www.who.int/hiv/pub/towards_universal_access_report_2008.pdf.
-
- Stringer JS, Zulu I, Levy J, Stringer EM, Mwango A, Chi BH, et al. Rapid scale-up of antiretroviral therapy at primary care sites in Zambia: feasibility and early outcomes. JAMA. 2006;296:782–793. - PubMed
-
- Ferradini L, Jeannin A, Pinoges L, Izopet J, Odhiambo D, Mankhambo L, et al. Scaling up of highly active antiretroviral therapy in a rural district of Malawi: an effectiveness assessment. Lancet. 2006;367:1335–1342. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
