

Dihydroartemisinin-piperaquine and artemether-lumefantrine for treating uncomplicated malaria in African children: a randomised, non-inferiority trial
- PMID: 19936217
- PMCID: PMC2776302
- DOI: 10.1371/journal.pone.0007871
Dihydroartemisinin-piperaquine and artemether-lumefantrine for treating uncomplicated malaria in African children: a randomised, non-inferiority trial
Abstract
Background: Artemisinin combination therapies (ACTs) are currently the preferred option for treating uncomplicated malaria. Dihydroartemisinin-piperaquine (DHA-PQP) is a promising fixed-dose ACT with limited information on its safety and efficacy in African children.
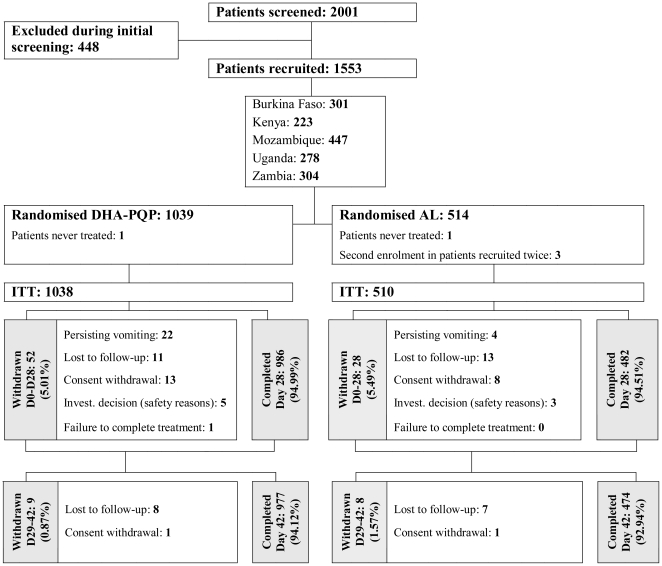
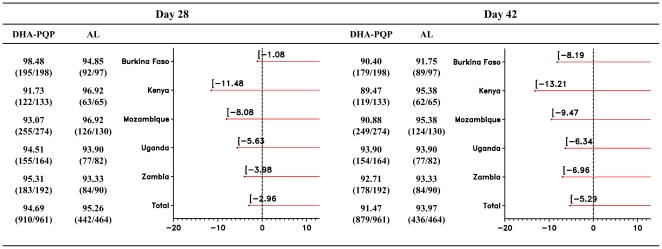
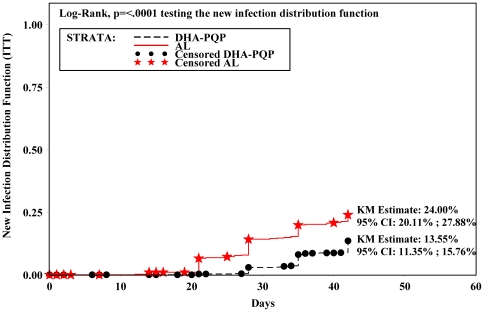
Methodology/principal findings: The non-inferiority of DHA-PQP versus artemether-lumefantrine (AL) in children 6-59 months old with uncomplicated P. falciparum malaria was tested in five African countries (Burkina Faso, Kenya, Mozambique, Uganda and Zambia). Patients were randomised (2:1) to receive either DHA-PQP or AL. Non-inferiority was assessed using a margin of -5% for the lower limit of the one-sided 97.5% confidence interval on the treatment difference (DHA-PQP vs. AL) of the day 28 polymerase chain reaction (PCR) corrected cure rate. Efficacy analysis was performed in several populations, and two of them are presented here: intention-to-treat (ITT) and enlarged per-protocol (ePP). 1553 children were randomised, 1039 receiving DHA-PQP and 514 AL. The PCR-corrected day 28 cure rate was 90.4% (ITT) and 94.7% (ePP) in the DHA-PQP group, and 90.0% (ITT) and 95.3% (ePP) in the AL group. The lower limits of the one-sided 97.5% CI of the difference between the two treatments were -2.80% and -2.96%, in the ITT and ePP populations, respectively. In the ITT population, the Kaplan-Meier estimate of the proportion of new infections up to Day 42 was 13.55% (95% CI: 11.35%-15.76%) for DHA-PQP vs 24.00% (95% CI: 20.11%-27.88%) for AL (p<0.0001).
Conclusions/significance: DHA-PQP is as efficacious as AL in treating uncomplicated malaria in African children from different endemicity settings, and shows a comparable safety profile. The occurrence of new infections within the 42-day follow up was significantly lower in the DHA-PQP group, indicating a longer post-treatment prophylactic effect.
Trial registration: Controlled-trials.com ISRCTN16263443.
Conflict of interest statement
Figures
References
-
- WHO. Guidelines for the Treatment of Malaria. 2006. Geneva: World Health Organization (Accessed November 2007, at http://www.who.int/malaria/docs/TreatmentGuidelines2006.pdf)
-
- WHO. The World malaria report. 2008. Geneva: World Health Organization (Accessed february 2009, at: http://apps.who.int/malaria/wmr2008/malaria2008.pdf)
-
- Price RN, Dorsey G, Nosten F. Antimalarial therapies in children from Papua New Guinea. N Engl J Med. 2009;360:1254; author reply 1255. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
