

The diagnosis of diverticulitis in outpatients: on what evidence?
- PMID: 19936848
- PMCID: PMC2844077
- DOI: 10.1007/s11605-009-1098-x
The diagnosis of diverticulitis in outpatients: on what evidence?
Abstract
Purpose: Diverticular disease is common in the outpatient setting; yet, rigorous study of diagnosis and management strategies is currently limited to hospitalized patients. Here, we characterize the clinical assessment generating the diagnostic label of diverticulitis in outpatients.
Methods: Encounters for diverticulitis were identified using ICD-9 diagnosis codes (562.11/562.13) from the electronic medical record system of a tertiary referral hospital and its regional clinics. The frequencies of various demographic and clinical variables were compared between patients presenting in the emergency room (ER) or outpatient Clinic.
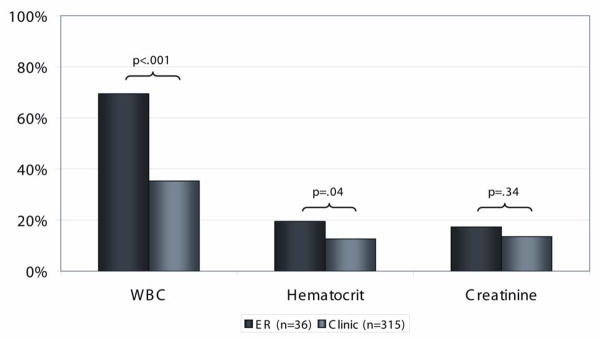
Results: Between 2003 and 2008, 820 inpatients and 2,576 outpatients met inclusion criteria (328 [13%] ER, 2,248 [87%] Clinic). Compared to ER patients, Clinic patients were less likely to undergo urgent abdominal/pelvic computed tomography (CT) scan (14% vs. 85%, p<.0001) or have an abnormal WBC count (35% vs. 69%, p<.0001). Twenty-four hour , including inpatient admission (30% ER vs. 3.5% Clinic, p<.0001) and colectomy (1.2% ER vs. 0.4% Clinic, p=0.08) were rare in both groups.
Conclusion: Diverticulitis in the outpatient setting is often characterized by infrequent use of CT scans, lack of leukocytosis, and rare need for urgent surgery or early admission. As this diagnostic label appears to be commonly applied without objective evidence, further study is needed to evaluate its validity.
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
