

Conventional and laparoscopic reversal of the Hartmann procedure: a review of literature
- PMID: 19936852
- PMCID: PMC2836249
- DOI: 10.1007/s11605-009-1084-3
Conventional and laparoscopic reversal of the Hartmann procedure: a review of literature
Abstract
Purpose: The aim of this study was to provide a systematic overview on both laparoscopic and conventional Hartmann reversal. Furthermore, the Hartmann procedure is reevaluated in the light of new emerging alternatives.
Methods: Medline, Ovid, EMBASE, and Cochrane database were searched for studies reporting on outcomes after Hartmann reversal.
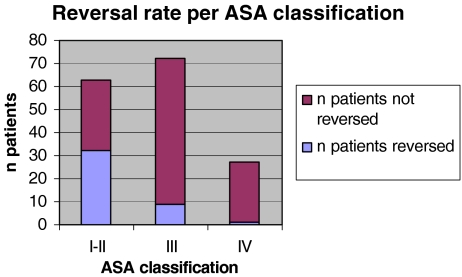
Results: Thirty-five studies were included in this review of which 30 were retrospective. A total of 6,249 patients with a mean age of 60 years underwent Hartmann reversal. Two thirds of patients were classified as American Society of Anesthesiologists (ASA) I-II. The mean reversal rate after a Hartmann procedure was 44%, and mean time interval between Hartmann procedure and Hartmann reversal was 7.5 months. The most frequent reported reasons for renouncing Hartmann reversal were high ASA classification and patients' refusal. The overall morbidity rate ranged from 3% to 50% (mean 16.3%) and mortality rate from 0% to 7.1% (mean 1%). Patients treated laparoscopically had a shorter hospital stay (6.9 vs. 10.7 days) and appeared to have lower mean morbidity rates compared to conventional surgery (12.2% vs. 20.3%).
Conclusion: Hartmann reversal carries a high risk on perioperative morbidity and mortality. The mean reversal rate is considerably low (44%). Laparoscopic reversal compares favorably to conventional; however, high level evidence is needed to determine whether it is superior.
Figures

References
-
- Roque-Castellano C, Marchena-Gomez J, Hemmersbach-Miller M, Acosta-Merida A, Rodriguez-Mendez A, Farina-Castro R, et al. Analysis of the factors related to the decision of restoring intestinal continuity after Hartmann’s procedure. Int J Colorectal Dis. 2007;22(9):1091–1096. doi: 10.1007/s00384-007-0272-4. - DOI - PubMed
-
- Vermeulen J, Coene PP, Van Hout NM, van der Harst E, Gosselink MP, Mannaerts GH, et al. Restoration of bowel continuity after surgery for acute perforated diverticulitis: should Hartmann’s procedure be considered a one-stage procedure? Colorectal Dis. 2008;11:619–624. doi: 10.1111/j.1463-1318.2008.01667.x. - DOI - PubMed
-
- Carcoforo P, Navarra G, Di Marco L, Occhionorelli S, Rocca T, Pollinzi V. Reversal of Hartmann’s procedure. Our experience. Ann Ital Chir. 1997;68(4):523–527. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
