

Assessment of future remnant liver function using hepatobiliary scintigraphy in patients undergoing major liver resection
- PMID: 19937195
- PMCID: PMC2809979
- DOI: 10.1007/s11605-009-1085-2
Assessment of future remnant liver function using hepatobiliary scintigraphy in patients undergoing major liver resection
Abstract
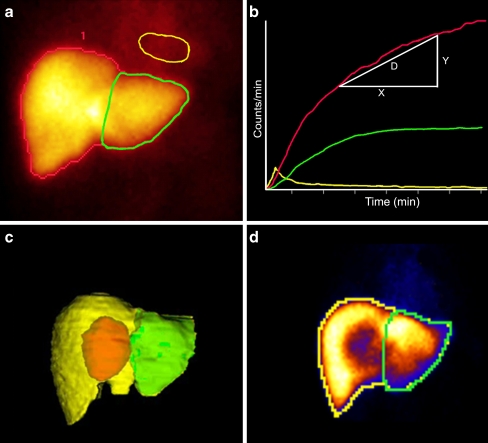
Background: (99m)Tc-mebrofenin hepatobiliary scintigraphy (HBS) was used as a quantitative method to evaluate liver function. The aim of this study was to compare future remnant liver function assessed by (99m)Tc-mebrofenin hepatobiliary scintigraphy with future remnant liver volume in the prediction of liver failure after major liver resection.
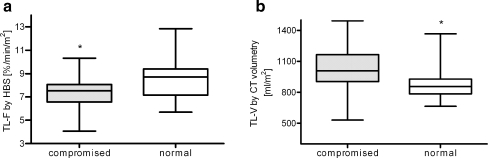
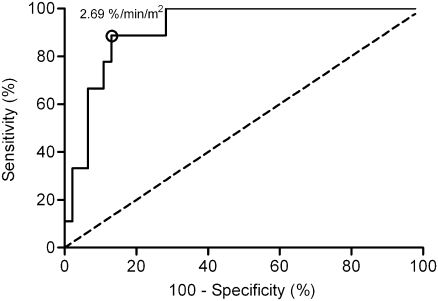
Methods: Computed tomography (CT) volumetry and (99m)Tc-mebrofenin hepatobiliary scintigraphy were performed prior to major resection in 55 high-risk patients, including 30 patients with parenchymal liver disease. Liver volume was expressed as percentage of total liver volume or as standardized future remnant liver volume. Receiver operating characteristic (ROC) curve analysis was performed to identify a cutoff value for future remnant liver function in predicting postoperative liver failure.
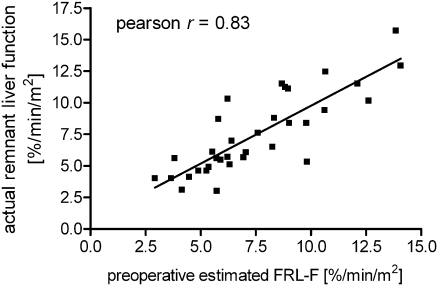
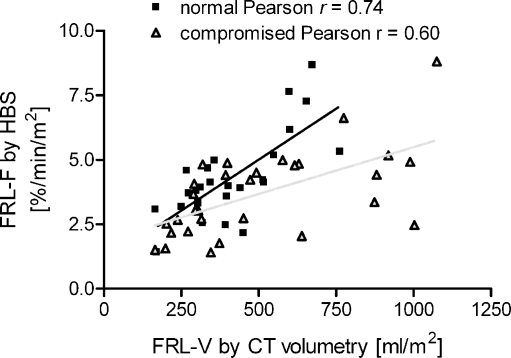
Results: Postoperative liver failure occurred in nine patients. A liver function cutoff value of 2.69%/min/m(2) was calculated by ROC curve analysis. (99m)Tc-mebrofenin hepatobiliary scintigraphy demonstrated better sensitivity, specificity, and positive and negative predictive value compared to future remnant liver volume. Using 99mTc-mebrofenin hepatobiliary scintigraphy, one cutoff value suffices in both compromised and noncompromised patients.
Conclusion: Preoperative (99m)Tc-mebrofenin hepatobiliary scintigraphy is a valuable technique to estimate the risk of postoperative liver failure. Especially in patients with uncertain quality of the liver parenchyma, (99m)Tc-mebrofenin HBS proved of more value than CT volumetry.
Figures
References
-
- Shirabe K, Shimada M, Gion T, Hasegawa H, Takenaka K, Utsunomiya T, Sugimachi K. Postoperative liver failure after major hepatic resection for hepatocellular carcinoma in the modern era with special reference to remnant liver volume. J Am Coll Surg. 1999;188:304–309. doi: 10.1016/S1072-7515(98)00301-9. - DOI - PubMed
-
- Kubota K, Makuuchi M, Kusaka K, Kobayashi T, Miki K, Hasegawa K, Harihara Y, Takayama T. Measurement of liver volume and hepatic functional reserve as a guide to decision-making in resectional surgery for hepatic tumors. Hepatology. 1997;26:1176–1181. - PubMed
-
- Vauthey JN, Chaoui A, Do KA, Bilimoria MM, Fenstermacher MJ, Charnsangavej C, Hicks M, Alsfasser G, Lauwers G, Hawkins IF, Caridi J. Standardized measurement of the future liver remnant prior to extended liver resection: methodology and clinical associations. Surgery. 2000;127:512–519. doi: 10.1067/msy.2000.105294. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
