

doi: 10.1007/s00247-009-1459-3.
Epub 2009 Nov 24.
MR imaging of the fetal brain
Affiliations
- PMID: 19937234
- PMCID: PMC3229879
- DOI: 10.1007/s00247-009-1459-3
Item in Clipboard
MR imaging of the fetal brain
Pediatr Radiol.
2010 Jan.
Abstract
Fetal MRI is clinically performed to evaluate the brain in cases where an abnormality is detected by prenatal sonography. These most commonly include ventriculomegaly, abnormalities of the corpus callosum, and abnormalities of the posterior fossa. Fetal MRI is also increasingly performed to evaluate fetuses who have normal brain findings on prenatal sonogram but who are at increased risk for neurodevelopmental abnormalities, such as complicated monochorionic twin pregnancies. This paper will briefly discuss the common clinical conditions imaged by fetal MRI as well as recent advances in fetal MRI research.
Figures
Axial SSFSE T2-W image in a 22 gestational week fetus demonstrates several hypointense nodules along the margin of the left lateral ventricle (arrows). This was confirmed on coronal SSFSE T2-W images (not shown) and is consistent with periventricular nodular heterotopia. (Reprinted with permission [2])

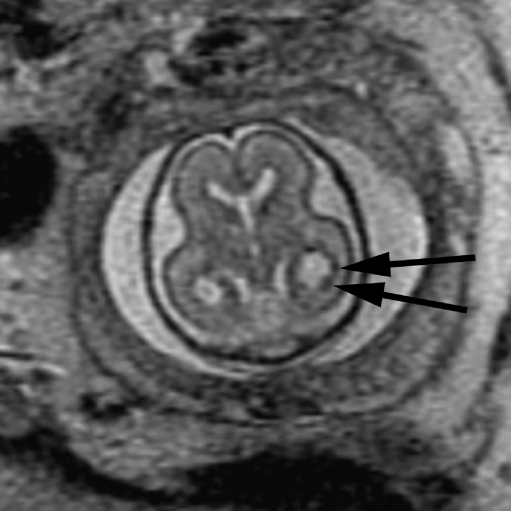
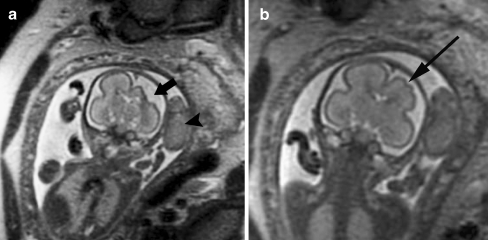
Coronal SSFSE T2-W image in a gestational week 26 fetus demonstrates several hypointense nodules along the margins of both lateral ventricles (arrows), consistent with subependymal nodules; these are indistinguishable from periventricular nodular heterotopia (see Fig. 1). A hypointense wedge-shaped area is seen extending from the margin of the left lateral ventricle to the developing cortex (arrowhead), consistent with transmantle dysplasia. Findings are consistent with tuberous sclerosis. (Reprinted with permission [2])
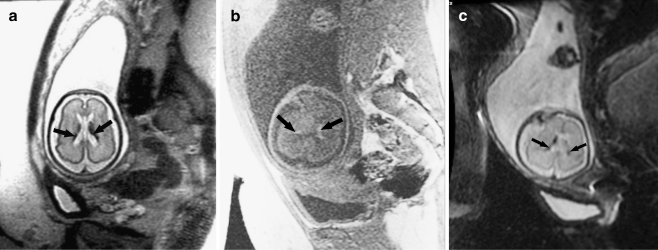
Bilateral germinal matrix hemorrhages in a 28 gestational week fetus. a Axial SSFSE T2-W image demonstrates abnormal hypointensity in the germinal matrix (which also appears too thick), consistent with bilateral germinal matrix hemorrhages (arrows). b Axial FMPSPGR T1-weighted image demonstrates T1 hyperintensity (which appears too thick) lining the lateral ventricles, also consistent with hemorrhage (arrows). c Axial echo-planar spin-echo T2-W image demonstrates marked hypointensity in similar regions, confirming the diagnosis of bilateral germinal matrix hemorrhages (arrows)
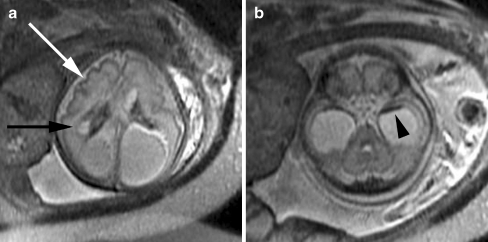
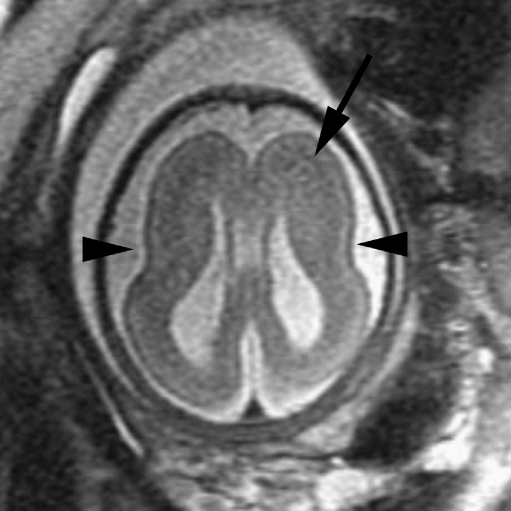
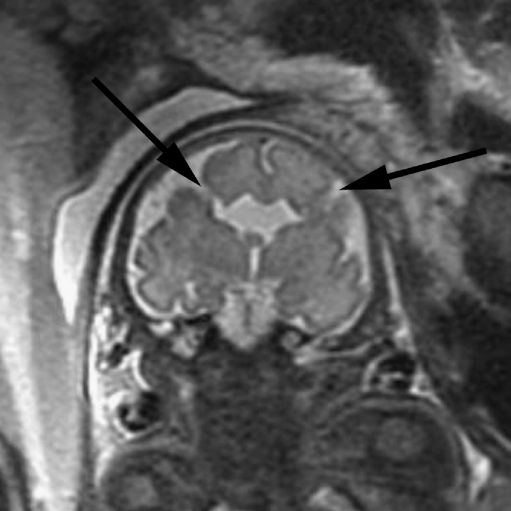
Cortical malformation and hemorrhage in a 27 gestational week fetus. a Axial SSFSE T2-W image demonstrates abnormal cortical infoldings of the frontal lobes, consistent with polymicrogyria (white arrow). Areas of cystic encephalomalacia with hemorrhage are also seen in the developing white matter (black arrow). b Intraventricular hemorrhage is seen layering in the temporal horns bilaterally (arrowhead). The patient was referred for ventriculomegaly and choroid plexus cysts detected on prenatal sonogram. (Reprinted with permission [2])
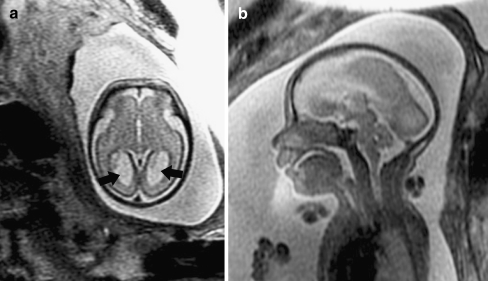
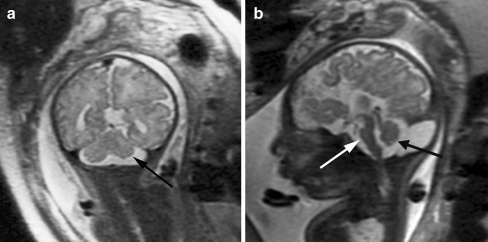
Absent corpus callosum in a 26 gestational week fetus referred for sonographically isolated mild ventriculomegaly. a Axial SSFSE T2-W image demonstrates dilatation of the posterior lateral ventricles (arrows). b Sagittal image demonstrates absent corpus callosum (compare with Fig. 8, where a normal corpus callosum is present)
Axial SSFSE T2-W image in a 34 gestational week fetus demonstrates abnormally shallow sylvian fissures (arrowheads) with absence of other sulci. A thick band of low signal intensity (arrow) is seen in the developing white matter, consistent with arrested migration of neurons. Findings are compatible with classical lissencephaly. (Reprinted with permission [119])
Coronal SSFSE T2WI in a 33 gestational week fetus demonstrates bilateral clefts extending from the ventricle to the subarachnoid space, consistent with open lip schizencephalic defects (arrows). The adjacent sulcal pattern is abnormal, consistent with polymicrogyria. The cavum septum pellucidum is absent. (Reprinted with permission [119])

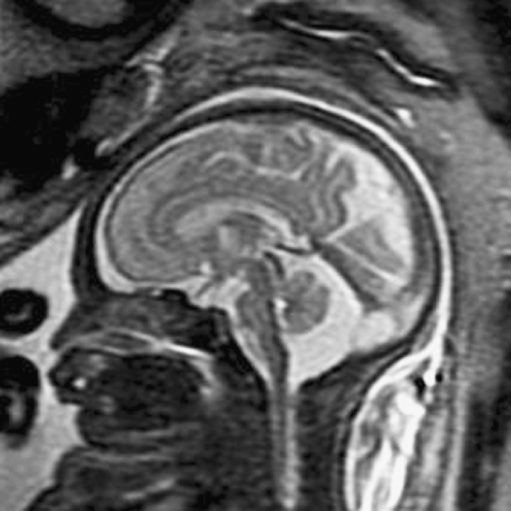
Midline sagittal SSFSE T2-W image demonstrates the normal appearance of the corpus callosum (arrow). Obtaining a 3-mm non-oblique midline sagittal image is important when evaluating the corpus callosum. (Reprinted with permission [119])
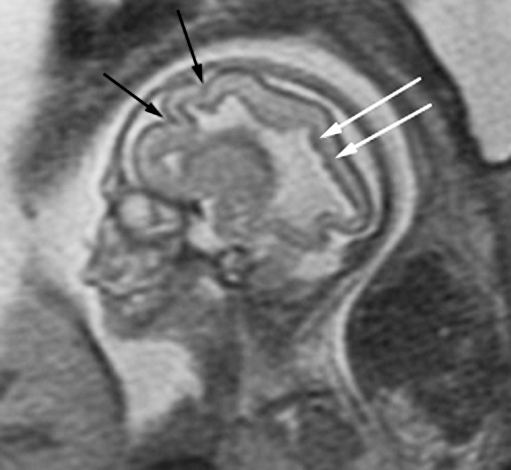
Sagittal SSFSE T2-W image in a 22 gestational week fetus demonstrates multiple abnormal infoldings of the cortex (black arrows). The lateral ventricle has an abnormal shape with multiple undulations along its margin and periventricular nodular heterotopia (white arrows). The multilayered pattern of the supratentorial parenchyma is absent. A diagnosis of Aicardi syndrome was confirmed postnatally. (Reprinted with permission [51])
Multiple abnormalities in a 36 gestational week fetus. a Coronal SSFSE T2-W image shows a small left cerebellar hemisphere (arrow). The sulcation pattern of both cerebral hemispheres is diffusely abnormal, with too many infoldings of the cortex. b Sagittal image demonstrates callosal agenesis, small pons (white arrow), small vermis (black arrow), and mega cisterna magna. (Reprinted with permission [51])
Sagittal SSFSE T2-W image in a 33 gestational week fetus demonstrates a large cisterna magna with a normal-appearing vermis, excluding the diagnosis of a Dandy-Walker malformation. (Reprinted with permission [119])
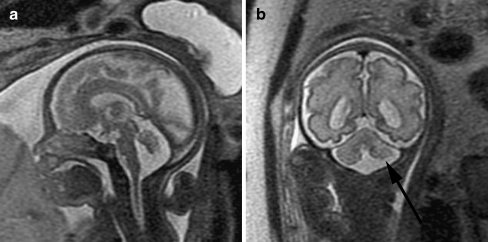
Dysmorphic cerebellum in a 29 gestational week fetus. a Sagittal SSFSE T2-W image demonstrates mild upward rotation of the vermis, which is slightly small inferiorly. b Coronal SSFSE T2-W image demonstrates small left cerebellum (arrow). (Reprinted with permission [119])
Chiari II malformation in a 22 gestational week fetus. a Sagittal SSFSE T2WI in a demonstrates a small posterior fossa with inferior displacement of the cerebellum, consistent with a Chiari II malformation. The corpus callosum is hypogenetic (arrow). There is diffuse effacement of the subarachnoid spaces, which is typically observed in Chiari II malformation. b Coronal SSFSE T2-W image in the same fetus demonstrates bilateral ventriculomegaly as well as two small hypointense nodules along the lateral margin of the atrium of the left lateral ventricle, consistent with periventricular nodular heterotopia (arrows). (Reprinted with permission [119])
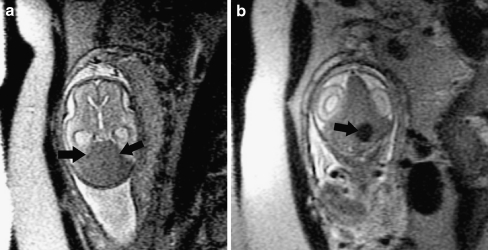
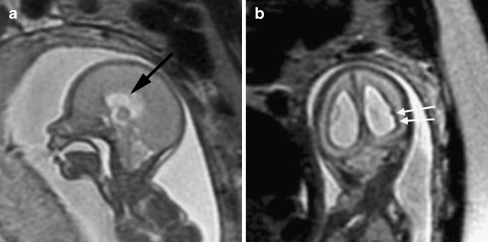
Dural sinus malformation with thrombosis in a 24 gestational week fetus. a Axial SSFSE T2-W image demonstrates a large intradural mass that is a slightly T2 hypointense (arrows). Findings are compatible with a dural sinus malformation. b Coronal SSFSE T2-W image demonstrates a focal ovoid area of T2 hypointensity within the dural sinus malformation, consistent with focal thrombus (arrow). (Reprinted with permission [119])

Axial SSFSE T2-W image in a 20 gestational week fetus demonstrates bilateral germinolytic cysts (arrows) consistent with prior germinal matrix injury. A portion of the demised twin is seen in the lower part of the image. Findings were confirmed on coronal image (not shown). (Reprinted with permission [81])
Encephalomalacia and malformation of cortical development in a 23 gestational week fetus. a Coronal SSFSE T2 image demonstrates encephalomalacia of the left frontal and parietal lobes (arrow). The demised twin is also seen (arrowhead). b Abnormal infoldings of the developing cortex are consistent with polymicrogyria (arrow). (Reprinted with permission [119])
References
-
- Garel C. MRI of the fetal brain: normal development and cerebral pathologies. Berlin: Springer; 2004.
-
- Prayer D, Kasprian G, Krampl E, et al. MRI of normal fetal brain development. Eur J Radiol. 2006;57:199–216. - PubMed
-
- Glenn OA. Normal development of the fetal brain by MRI. Semin Perinatol. 2009;33:208–219. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
