

The plasma lipidomic signature of nonalcoholic steatohepatitis
- PMID: 19937697
- PMCID: PMC5031239
- DOI: 10.1002/hep.23229
The plasma lipidomic signature of nonalcoholic steatohepatitis
Abstract
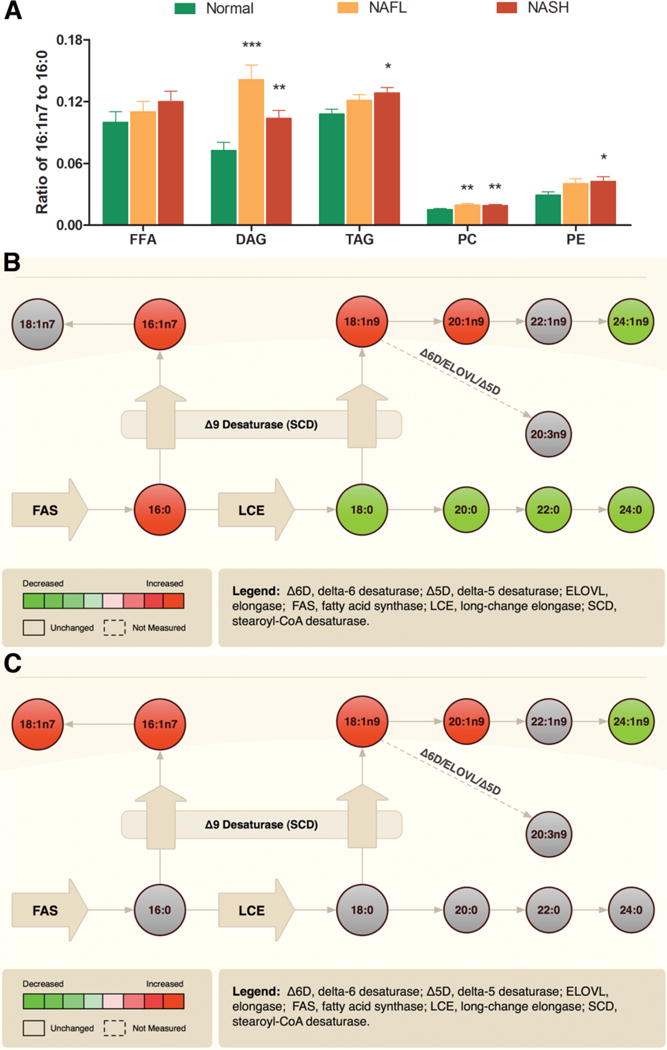
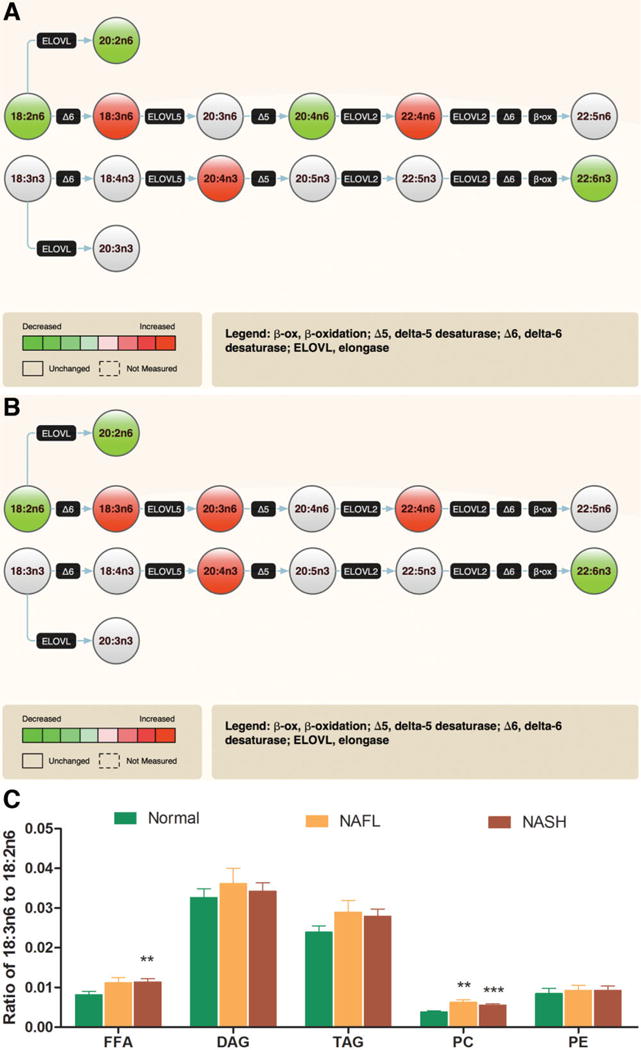
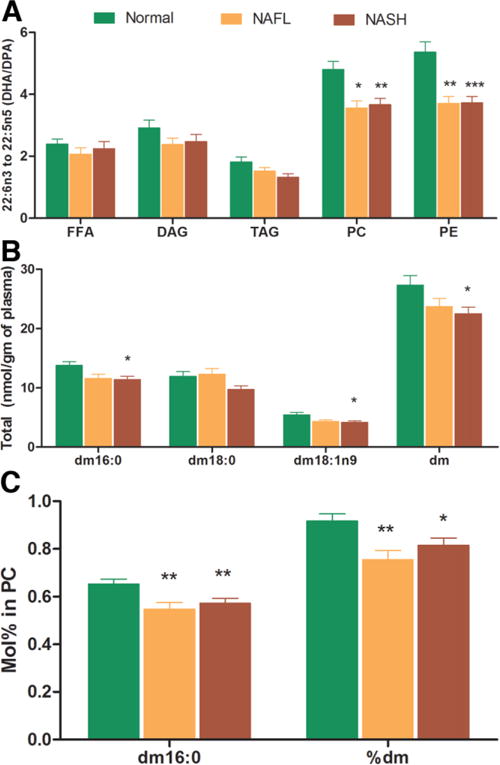
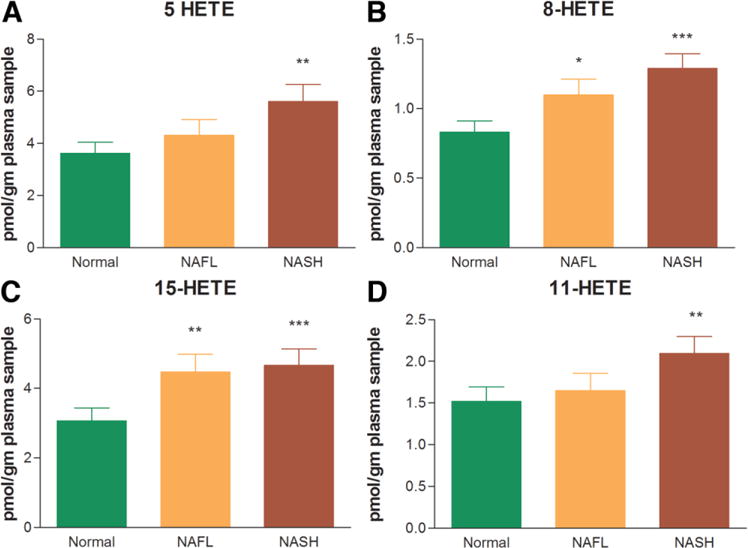
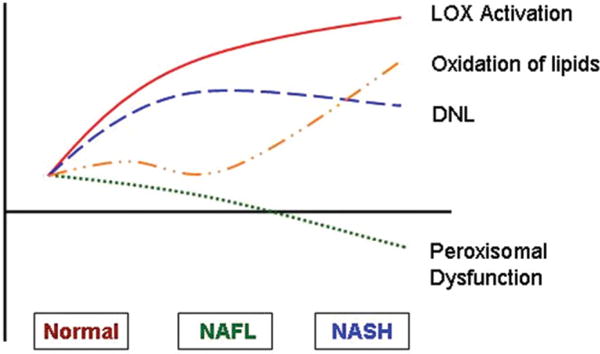
Specific alterations in hepatic lipid composition characterize the spectrum of nonalcoholic fatty liver disease (NAFLD), which extends from nonalcoholic fatty liver (NAFL) to nonalcoholic steatohepatitis (NASH). However, the plasma lipidome of NAFLD and whether NASH has a distinct plasma lipidomic signature are unknown. A comprehensive analysis of plasma lipids and eicosanoid metabolites quantified by mass spectrometry was performed in NAFL (n = 25) and NASH (n = 50) subjects and compared with lean normal controls (n = 50). The key findings include significantly increased total plasma monounsaturated fatty acids driven by palmitoleic (16:1 n7) and oleic (18:1 n9) acids content (P < 0.01 for both acids in both NAFL and NASH). The levels of palmitoleic acid, oleic acid, and palmitoleic acid to palmitic acid (16:0) ratio were significantly increased in NAFLD across multiple lipid classes. Linoleic acid (8:2n6) was decreased (P < 0.05), with a concomitant increase in gamma-linolenic (18:3n6) and dihomo gamma-linolenic (20:3n6) acids in both NAFL and NASH (P < 0.001 for most lipid classes). The docosahexanoic acid (22:6 n3) to docosapentenoic acid (22:5n3) ratio was significantly decreased within phosphatidylcholine (PC), and phosphatidylethanolamine (PE) pools, which was most marked in NASH subjects (P < 0.01 for PC and P < 0.001 for PE). The total plasmalogen levels were significantly decreased in NASH compared with controls (P < 0.05). A stepwise increase in lipoxygenase (LOX) metabolites 5(S)-hydroxyeicosatetraenoic acid (5-HETE), 8-HETE, and 15-HETE characterized progression from normal to NAFL to NASH. The level of 11-HETE, a nonenzymatic oxidation product of arachidonic (20:4) acid, was significantly increased in NASH only.
Conclusions: Although increased lipogenesis, desaturases, and LOX activities characterize NAFL and NASH, impaired peroxisomal polyunsaturated fatty acid (PUFA) metabolism and nonenzymatic oxidation is associated with progression to NASH.
Conflict of interest statement
Potential conflict of interest: Dr. Wiest is a consultant for and Dr. Watkins owns stock in Lipomics.
Figures

Comment in
-
Lipidomic dissection of nonalcoholic steatohepatitis: moving beyond foie gras to fat traffic.Hepatology. 2010 Jan;51(1):4-7. doi: 10.1002/hep.23458. Hepatology. 2010. PMID: 20034031 No abstract available.
References
-
- Browning JD, Szczepaniak LS, Dobbins R, Nuremberg P, Horton JD, Cohen JC, et al. Prevalence of hepatic steatosis in an urban population in the United States: impact of ethnicity. Hepatology. 2004;40:1387–1395. - PubMed
-
- Contos MJ, Sanyal AJ. The clinicopathologic spectrum and management of nonalcoholic fatty liver disease. Adv Anat Pathol. 2002;9:37–51. - PubMed
-
- Ekstedt M, Franzen LE, Mathiesen UL, Thorelius L, Holmqvist M, Bodemar G, et al. Long-term follow-up of patients with NAFLD and elevated liver enzymes. Hepatology. 2006;44:865–873. - PubMed
-
- Ludwig J, Viggiano TR, McGill DB, Oh BJ. Nonalcoholic steatohepatitis: Mayo Clinic experiences with a hitherto unnamed disease. Mayo Clin Proc. 1980;55:434–438. - PubMed
-
- Sanyal AJ, Campbell-Sargent C, Mirshahi F, Rizzo WB, Contos MJ, Sterling RK, et al. Nonalcoholic steatohepatitis: association of insulin resistance and mitochondrial abnormalities. Gastroenterology. 2001;120:1183–1192. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical