

Foot posture influences the electromyographic activity of selected lower limb muscles during gait
- PMID: 19939283
- PMCID: PMC2788543
- DOI: 10.1186/1757-1146-2-35
Foot posture influences the electromyographic activity of selected lower limb muscles during gait
Abstract
Background: Some studies have found that flat-arched foot posture is related to altered lower limb muscle function compared to normal- or high-arched feet. However, the results from these studies were based on highly selected populations such as those with rheumatoid arthritis. Therefore, the objective of this study was to compare lower limb muscle function of normal and flat-arched feet in people without pain or disease.
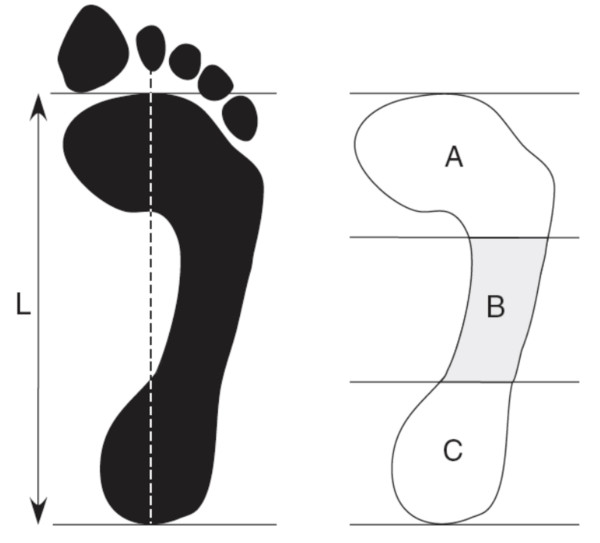
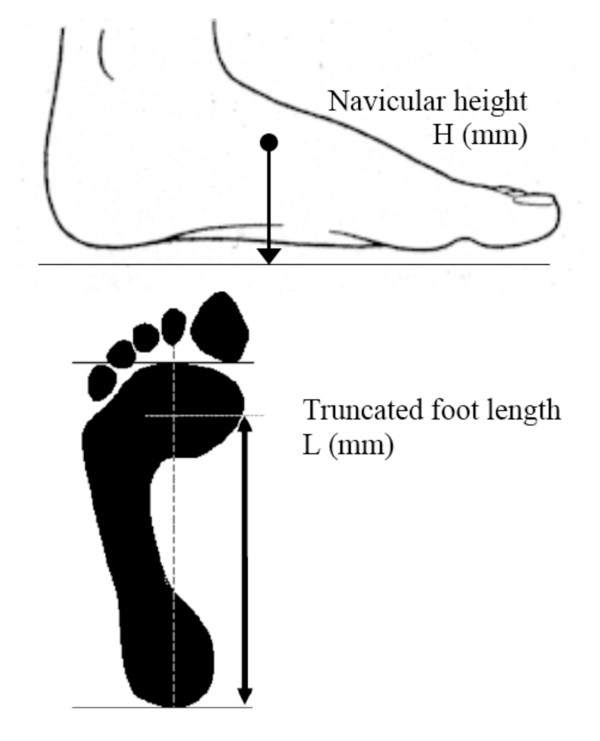
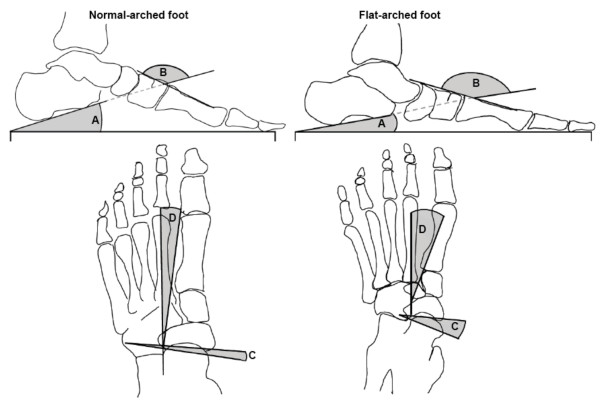
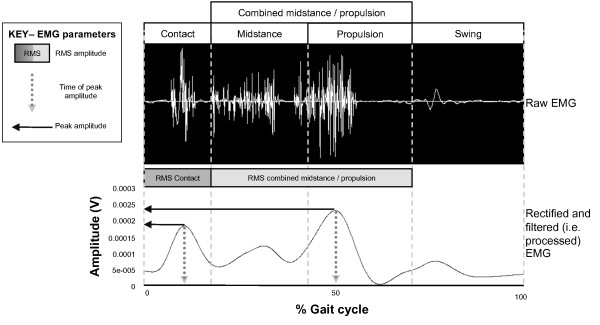
Methods: Sixty adults aged 18 to 47 years were recruited to this study. Of these, 30 had normal-arched feet (15 male and 15 female) and 30 had flat-arched feet (15 male and 15 female). Foot posture was classified using two clinical measurements (the arch index and navicular height) and four skeletal alignment measurements from weightbearing foot x-rays. Intramuscular fine-wire electrodes were inserted into tibialis posterior and peroneus longus under ultrasound guidance, and surface EMG activity was recorded from tibialis anterior and medial gastrocnemius while participants walked barefoot at their self-selected comfortable walking speed. Time of peak amplitude, peak and root mean square (RMS) amplitude were assessed from stance phase EMG data. Independent samples t-tests were performed to assess for significant differences between the normal- and flat-arched foot posture groups.
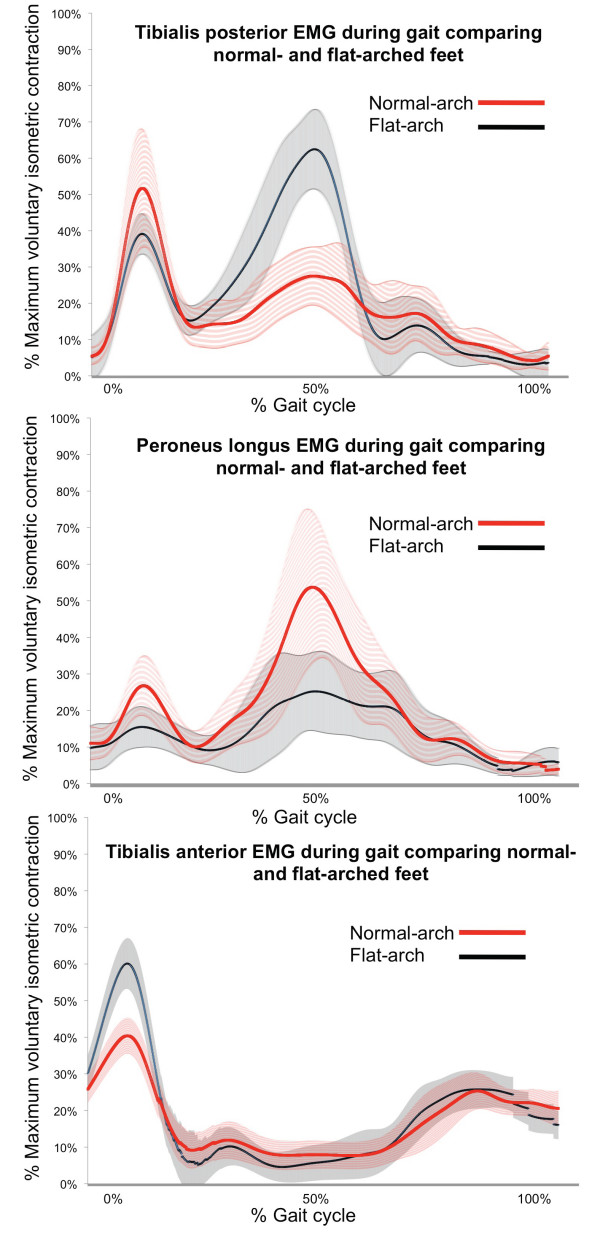
Results: During contact phase, the flat-arched group exhibited increased activity of tibialis anterior (peak amplitude; 65 versus 46% of maximum voluntary isometric contraction) and decreased activity of peroneus longus (peak amplitude; 24 versus 37% of maximum voluntary isometric contraction). During midstance/propulsion, the flat-arched group exhibited increased activity of tibialis posterior (peak amplitude; 86 versus 60% of maximum voluntary isometric contraction) and decreased activity of peroneus longus (RMS amplitude; 25 versus 39% of maximum voluntary isometric contraction). Effect sizes for these significant findings ranged from 0.48 to 1.3, representing moderate to large differences in muscle activity between normal-arched and flat-arched feet.
Conclusion: Differences in muscle activity in people with flat-arched feet may reflect neuromuscular compensation to reduce overload of the medial longitudinal arch. Further research is required to determine whether these differences in muscle function are associated with injury.
Figures
References
-
- Burns J, Keenan A-M, Redmond A. Foot Type and overuse onjury in triathletes. J Am Podiatr Med Assoc. 2005;95:235–241. - PubMed
LinkOut - more resources
Full Text Sources
Medical
