

Rates of virological failure in patients treated in a home-based versus a facility-based HIV-care model in Jinja, southeast Uganda: a cluster-randomised equivalence trial
- PMID: 19939445
- PMCID: PMC2806484
- DOI: 10.1016/S0140-6736(09)61674-3
Rates of virological failure in patients treated in a home-based versus a facility-based HIV-care model in Jinja, southeast Uganda: a cluster-randomised equivalence trial
Abstract
Background: Identification of new ways to increase access to antiretroviral therapy in Africa is an urgent priority. We assessed whether home-based HIV care was as effective as was facility-based care.
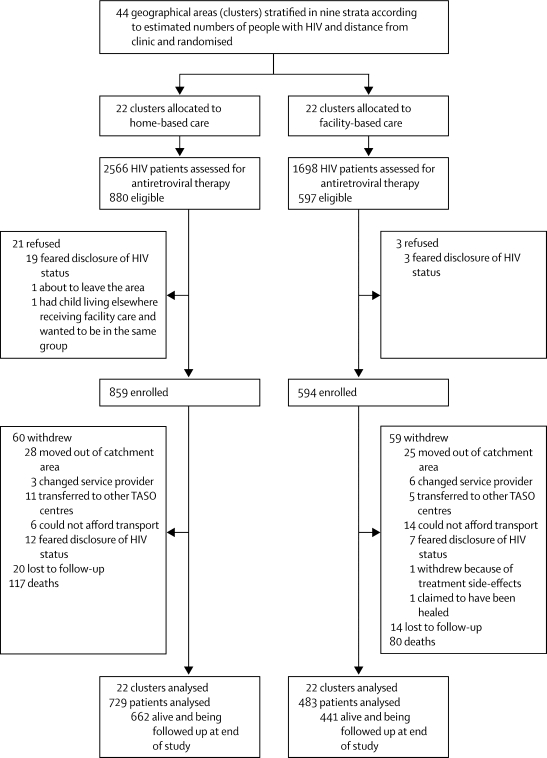
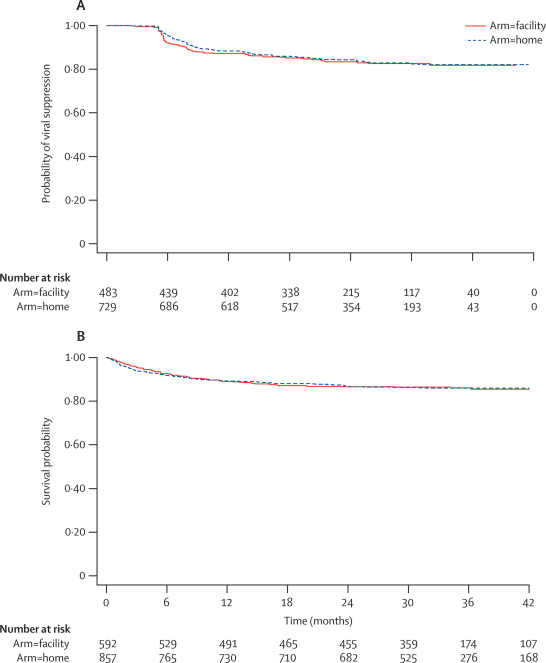
Methods: We undertook a cluster-randomised equivalence trial in Jinja, Uganda. 44 geographical areas in nine strata, defined according to ratio of urban and rural participants and distance from the clinic, were randomised to home-based or facility-based care by drawing sealed cards from a box. The trial was integrated into normal service delivery. All patients with WHO stage IV or late stage III disease or CD4-cell counts fewer than 200 cells per microL who started antiretroviral therapy between Feb 15, 2005, and Dec 19, 2006, were eligible, apart from those living on islands. Follow-up continued until Jan 31, 2009. The primary endpoint was virological failure, defined as RNA more than 500 copies per mL after 6 months of treatment. The margin of equivalence was 9% (equivalence limits 0.69-1.45). Analyses were by intention to treat and adjusted for baseline CD4-cell count and study stratum. This trial is registered at http://isrctn.org, number ISRCTN 17184129.
Findings: 859 patients (22 clusters) were randomly assigned to home and 594 (22 clusters) to facility care. During the first year, 93 (11%) receiving home care and 66 (11%) receiving facility care died, 29 (3%) receiving home and 36 (6%) receiving facility care withdrew, and 8 (1%) receiving home and 9 (2%) receiving facility care were lost to follow-up. 117 of 729 (16%) in home care had virological failure versus 80 of 483 (17%) in facility care: rates per 100 person-years were 8.19 (95% CI 6.84-9.82) for home and 8.67 (6.96-10.79) for facility care (rate ratio [RR] 1.04, 0.78-1.40; equivalence shown). Two patients from each group were immediately lost to follow-up. Mortality rates were similar between groups (0.95 [0.71-1.28]). 97 of 857 (11%) patients in home and 75 of 592 (13%) in facility care were admitted at least once (0.91, 0.64-1.28).
Interpretation: This home-based HIV-care strategy is as effective as is a clinic-based strategy, and therefore could enable improved and equitable access to HIV treatment, especially in areas with poor infrastructure and access to clinic care.
Copyright 2009 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
ART in rural Uganda--efficient scale-up with home-based care?Lancet. 2009 Dec 19;374(9707):2034-2035. doi: 10.1016/S0140-6736(09)62027-4. Epub 2009 Nov 24. Lancet. 2009. PMID: 19939444 No abstract available.
References
-
- WHO . Towards universal access: scaling up priority HIV/AIDS interventions in the health sector: progress report 2008. Report by the Secretariat. WHO; Geneva: 2008.
-
- United Nations General Assembly . Political Declaration on HIV/AIDS. United Nations; New York: 2006. http://www.unaids.org/en/AboutUNAIDS/Goals/UNGASS (United Nations General Assembly document 60/262. (accessed May 1, 2009).
-
- WHO . The World Health Report: primary care now more than ever. WHO; Geneva: 2008.
-
- Hardon AP, Akurut D, Comoro C. Hunger, waiting time and transport costs: time to confront challenges to ART adherence in Africa. AIDS Care. 2007;19:658–665. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
