

Rituximab, B-lymphocyte depletion, and preservation of beta-cell function
- PMID: 19940299
- PMCID: PMC6410357
- DOI: 10.1056/NEJMoa0904452
Rituximab, B-lymphocyte depletion, and preservation of beta-cell function
Abstract
Background: The immunopathogenesis of type 1 diabetes mellitus is associated with T-lymphocyte autoimmunity. However, there is growing evidence that B lymphocytes play a role in many T-lymphocyte-mediated diseases. It is possible to achieve selective depletion of B lymphocytes with rituximab, an anti-CD20 monoclonal antibody. This phase 2 study evaluated the role of B-lymphocyte depletion in patients with type 1 diabetes.
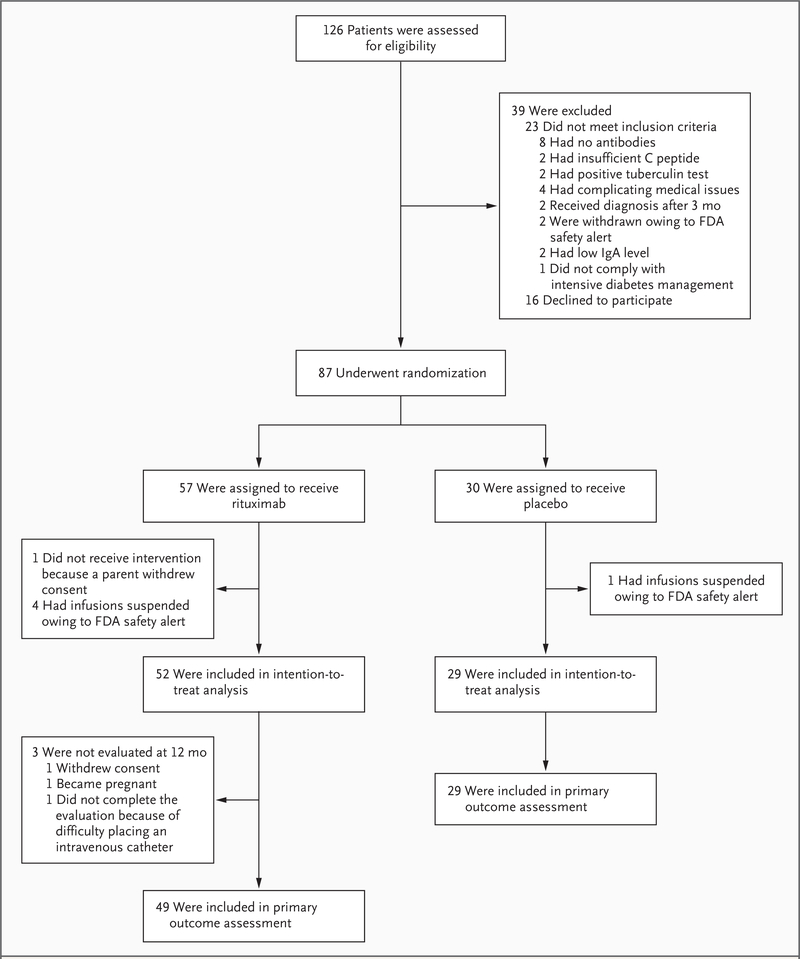
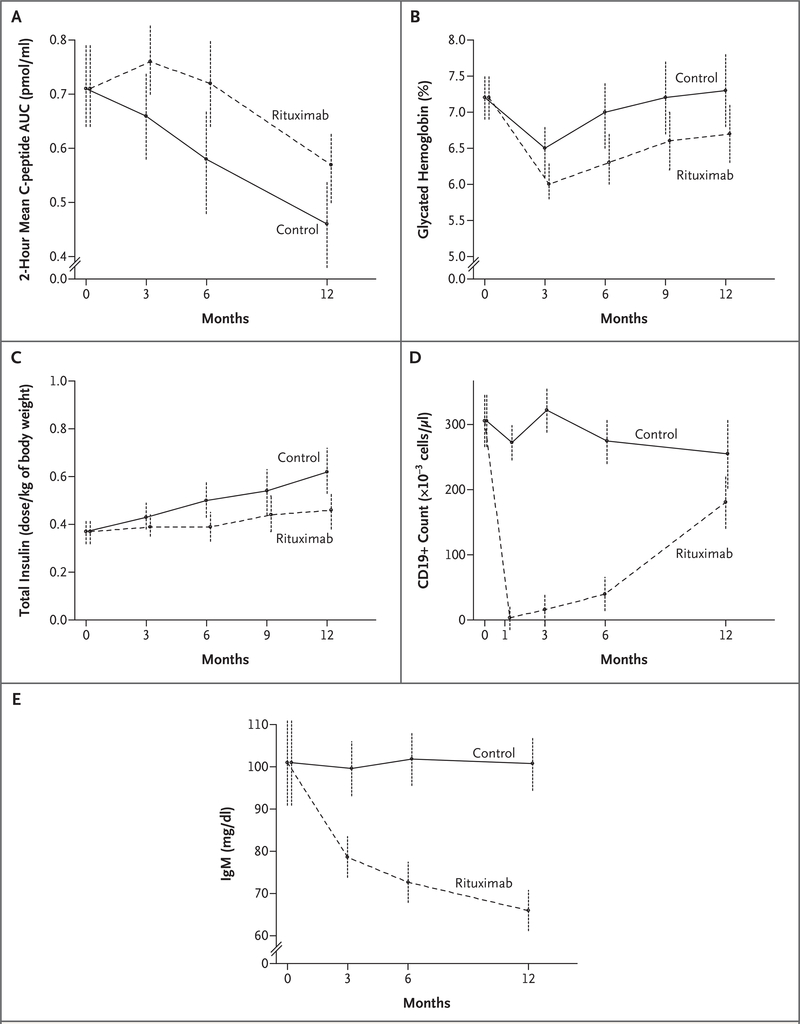
Methods: We conducted a randomized, double-blind study in which 87 patients between 8 and 40 years of age who had newly diagnosed type 1 diabetes were assigned to receive infusions of rituximab or placebo on days 1, 8, 15, and 22 of the study. The primary outcome, assessed 1 year after the first infusion, was the geometric mean area under the curve (AUC) for the serum C-peptide level during the first 2 hours of a mixed-meal tolerance test. Secondary outcomes included safety and changes in the glycated hemoglobin level and insulin dose.
Results: At 1 year, the mean AUC for the level of C peptide was significantly higher in the rituximab group than in the placebo group. The rituximab group also had significantly lower levels of glycated hemoglobin and required less insulin. Between 3 months and 12 months, the rate of decline in C-peptide levels in the rituximab group was significantly less than that in the placebo group. CD19+ B lymphocytes were depleted in patients in the rituximab group, but levels increased to 69% of baseline values at 12 months. More patients in the rituximab group than in the placebo group had adverse events, mostly grade 1 or grade 2, after the first infusion. The reactions appeared to be minimal with subsequent infusions. There was no increase in infections or neutropenia with rituximab.
Conclusions: A four-dose course of rituximab partially preserved beta-cell function over a period of 1 year in patients with type 1 diabetes. The finding that B lymphocytes contribute to the pathogenesis of type 1 diabetes may open a new pathway for exploration in the treatment of patients with this condition. (ClinicalTrials.gov number, NCT00279305.)
2009 Massachusetts Medical Society
Figures
Comment in
-
Rituximab, B-lymphocyte depletion, and beta-cell function.N Engl J Med. 2010 Feb 25;362(8):761; author reply 761. doi: 10.1056/NEJMc0912877. N Engl J Med. 2010. PMID: 20181981 No abstract available.
References
-
- The Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993;329: 977–86. - PubMed
-
- Schernthaner G Progress in the immunointervention of type-1 diabetes mellitus. Horm Metab Res 1995;27:547–54. - PubMed
-
- Mahon JL, Dupre J, Stiller CR. Lessons learned from the use of cyclosporine for insulin-dependent diabetes mellitus: the case for immunotherapy for insulin-dependent diabetics having residual insulin secretion. Ann N Y Acad Sci 1993;696:351–63. - PubMed
-
- Feutren G, Mihatsch M. Risk factors for cyclosporine-induced nephropathy in patients with autoimmune diseases. N Engl J Med 1992;326:1654–60. - PubMed
-
- Keymeulen B, Vandemeulebroucke E, Ziegler AG, et al. Insulin needs after CD3-antibody therapy in new-onset type 1 diabetes. N Engl J Med 2005;352:2598–608. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical