

Osteoradionecrosis of the hyoid bone: imaging findings
- PMID: 19942694
- PMCID: PMC7964243
- DOI: 10.3174/ajnr.A1892
Osteoradionecrosis of the hyoid bone: imaging findings
Abstract
Background and purpose: ORN is a postradiation complication that has been well-documented in the medical literature. Most cases in the head and neck have been described in the mandible or larynx. Only a handful of cases in the hyoid bone are documented, all in the clinical literature. Our purpose is to present the clinical and imaging features of ORN involving the hyoid bone.
Materials and methods: We present a case series of 13 patients with imaging findings highly suggestive of hyoid ORN after radiation therapy for head and neck cancers, in which we observed progressive features of hyoid disruption along with adjacent soft-tissue ulceration.
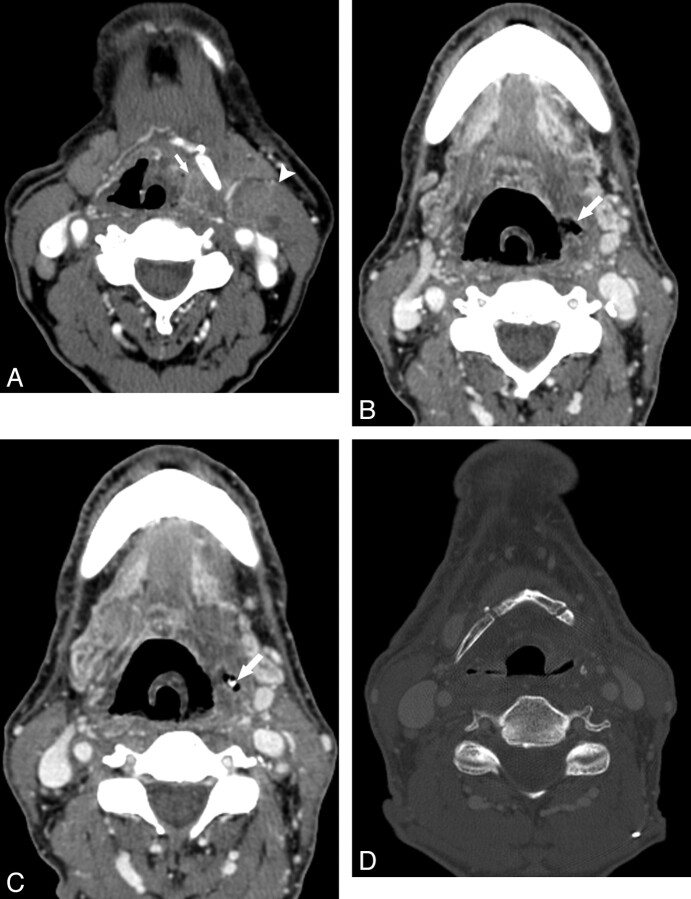
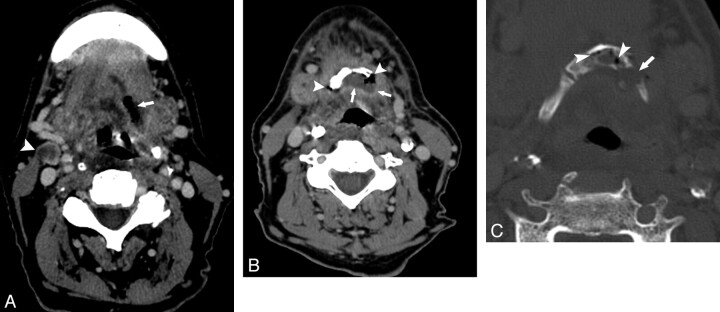
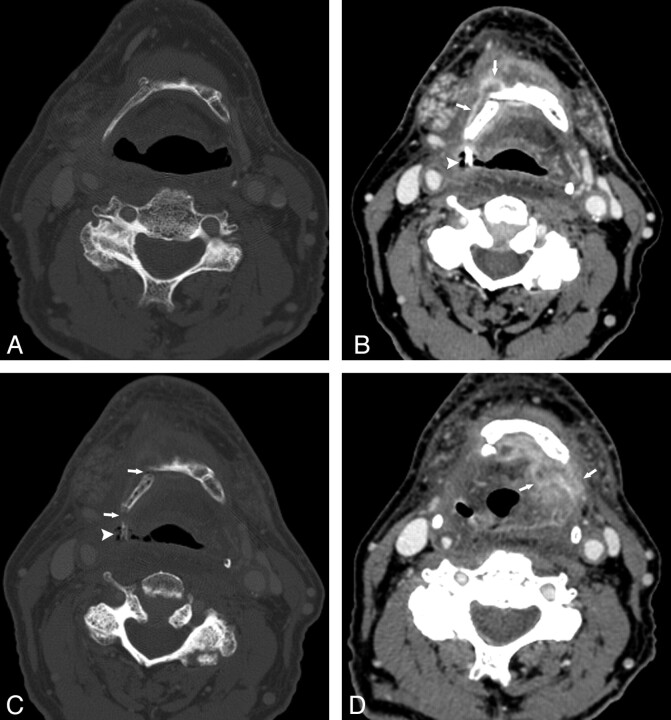
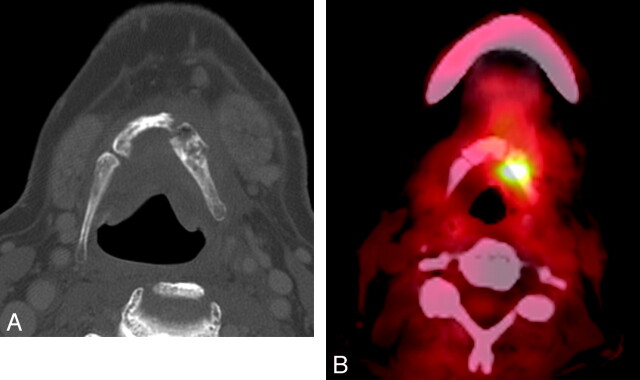
Results: Pretreatment imaging, when available, showed a normal hyoid. Typical postradiation imaging findings included an initial tongue base ulcerative lesion with air approaching the hyoid bone, and subsequent observation of hyoid fragmentation, often with intraosseous or peri-hyoid air and the absence of associated mass-like enhancement.
Conclusions: Findings of hyoid fragmentation, cortical disruption, and soft tissue or intraosseous air in the postradiation therapy patient should strongly suggest the diagnosis of hyoid ORN. It is important recognize this entity because the diagnosis may preclude potentially harmful diagnostic intervention and allow more appropriate therapy.
Figures

Similar articles
-
Osteoradionecrosis of the hyoid presenting as acute airway compromise.Head Neck. 2021 Sep;43(9):E41-E44. doi: 10.1002/hed.26790. Epub 2021 Jul 5. Head Neck. 2021. PMID: 34227172
-
Osteoradionecrosis of the hyoid bone complicated by pharyngocutaneous fistula: A case report and literature review.Am J Otolaryngol. 2019 Mar-Apr;40(2):314-318. doi: 10.1016/j.amjoto.2018.12.006. Epub 2018 Dec 7. Am J Otolaryngol. 2019. PMID: 30558897 Review.
-
Osteoradionecrosis of the hyoid bone after intra-arterial chemoradiotherapy for oropharyngeal cancer: MR imaging findings.Cancer Imaging. 2017 Jul 27;17(1):22. doi: 10.1186/s40644-017-0123-7. Cancer Imaging. 2017. PMID: 28750685 Free PMC article.
-
18F-FDG PET/CT in Osteoradionecrosis of the Hyoid.Clin Nucl Med. 2021 Jan;46(1):e49-e50. doi: 10.1097/RLU.0000000000003298. Clin Nucl Med. 2021. PMID: 32956123
-
Osteoradionecrosis of the hyoid bone: a report of 3 cases.Am J Otolaryngol. 1999 Nov-Dec;20(6):400-4. doi: 10.1016/s0196-0709(99)90081-9. Am J Otolaryngol. 1999. PMID: 10609486 Review.
Cited by
-
Imaging of the Head and Neck following Radiation Treatment.Patholog Res Int. 2011;2011:607820. doi: 10.4061/2011/607820. Epub 2011 May 11. Patholog Res Int. 2011. PMID: 21660277 Free PMC article.
-
Post-treatment appearances, pitfalls, and patterns of failure in head and neck cancer on FDG PET/CT imaging.Indian J Nucl Med. 2014 Jul;29(3):151-7. doi: 10.4103/0972-3919.136564. Indian J Nucl Med. 2014. PMID: 25210280 Free PMC article.
-
Osteoradionecrosis after radiation therapy for head and neck cancer: differentiation from recurrent disease with CT and PET/CT imaging.AJNR Am J Neuroradiol. 2014 Jul;35(7):1405-11. doi: 10.3174/ajnr.A3879. Epub 2014 Mar 13. AJNR Am J Neuroradiol. 2014. PMID: 24627451 Free PMC article.
-
Osteoradionecrosis of the hyoid bone--a novel application of the Sonopet ultrasonic aspirator.BMJ Case Rep. 2014 Sep 22;2014:bcr2014205682. doi: 10.1136/bcr-2014-205682. BMJ Case Rep. 2014. PMID: 25246467 Free PMC article.
-
Superimposed infection in mandibular osteoradionecrosis: diagnosis and outcomes.J Comput Assist Tomogr. 2012 Nov-Dec;36(6):725-31. doi: 10.1097/RCT.0b013e3182702f09. J Comput Assist Tomogr. 2012. PMID: 23192211 Free PMC article.
References
-
- Bedwinick JM, Shukovsky LJ, Fletcher GH, et al. . Osteonecrosis in patients treated with definitive radiotherapy for squamous cell carcinomas of the oral cavity and naso- and oro-pharynx. Radiology 1976; 119: 665–67 - PubMed
-
- MacDougall JA, Evans AM, Lindsay RK. Osteoradionecrosis of the mandible and its treatment. Am J Surg 1963; 106: 816–18 - PubMed
-
- Bhatia PL, Dutta NK, Sanasam JC. Osteonecrosis of hyoid bone and thyroid cartilage. Arch Otolaryngol 1979; 105: 553–54 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical