

Negative CT angiography findings in patients with spontaneous subarachnoid hemorrhage: When is digital subtraction angiography still needed?
- PMID: 19942709
- PMCID: PMC7964209
- DOI: 10.3174/ajnr.A1884
Negative CT angiography findings in patients with spontaneous subarachnoid hemorrhage: When is digital subtraction angiography still needed?
Abstract
Background and purpose: CTA is becoming the frontline modality to reveal aneurysms in patients with SAH. However, in about 20% of SAH patients no aneurysm is found. In these cases, intra-arterial DSA is still performed. Our aim was to evaluate whether negative findings on CTA can reliably exclude aneurysms in patients with acute SAH.
Materials and methods: We conducted a retrospective analysis of all negative findings on CTAs performed from 2005 to 2009 in patients with spontaneous SAH. Findings were compared with DSA. CTAs were performed with a 64-section multidetector row CT scanner.
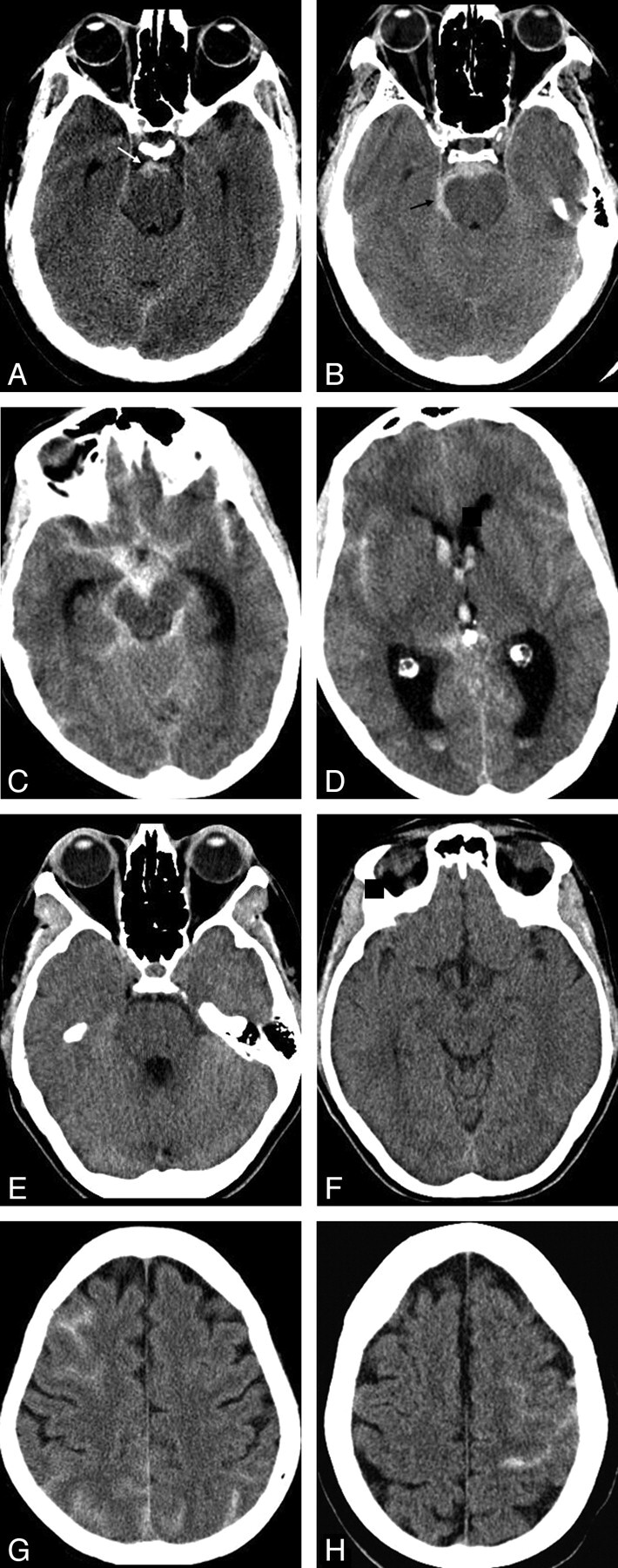
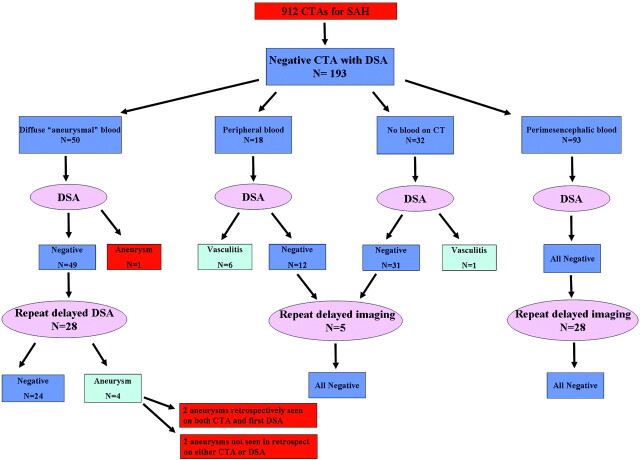
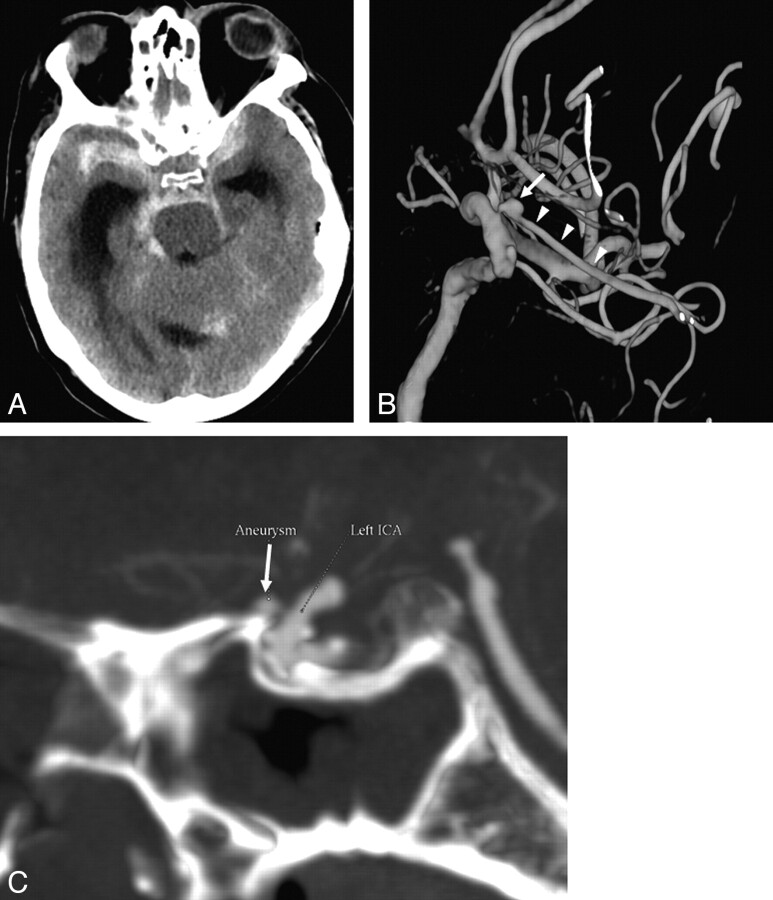
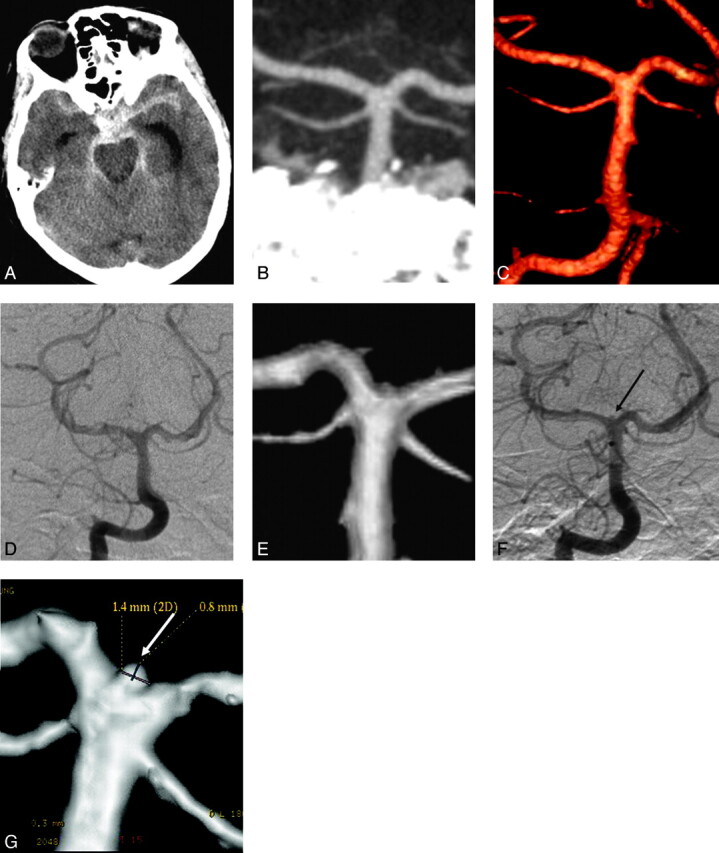
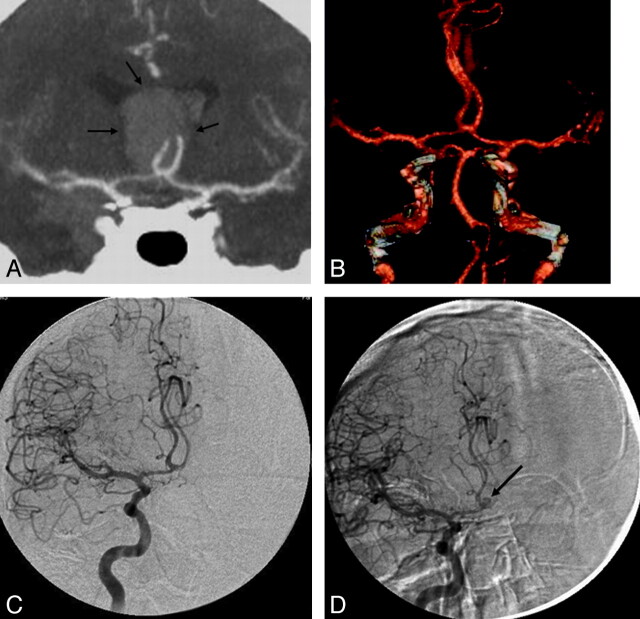
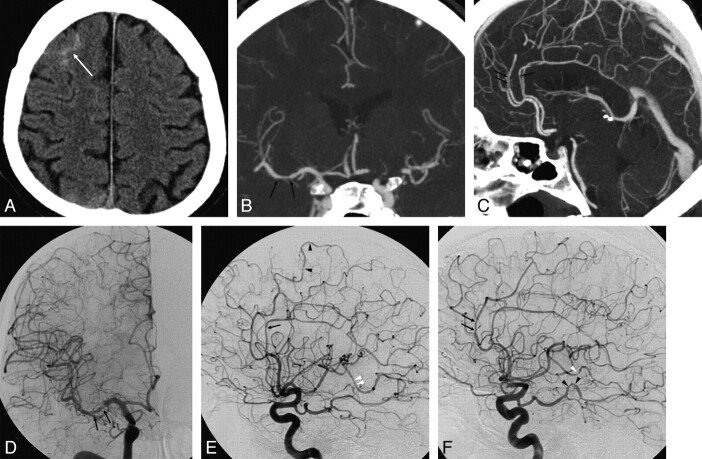
Results: One hundred ninety-three patients with SAH and negative findings on CTA who underwent subsequent DSA were identified. The distribution of blood on unenhanced CT was the following: PMH in 93 patients, diffuse aneurysmal pattern in 50, no blood on CT (xanthochromic LP) in 32, and peripheral sulcal distribution in 18. All patients with PMH had negative findings on DSA. One patient with no blood on CT had vasculitis on DSA. Six of 18 (33%) patients with peripheral blood had vasculitis on DSA. Three of these were also diagnosed by CTA. All except 1 patient with diffuse aneurysmal blood had negative findings on DSA. One patient was diagnosed with an aneurysm on DSA (1/50, 0.5%). Repeat delayed DSA performed in 28 of these patients revealed a small aneurysm in 4 (14%). Five patients had a complication of DSA (2.6%); 1 was a clinical stroke (0.5%).
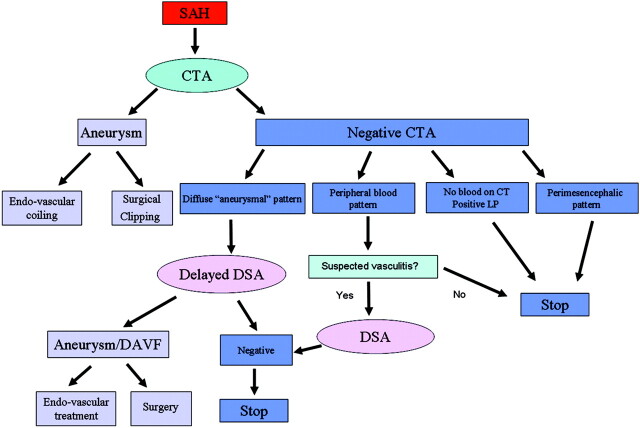
Conclusions: In patients with SAH, negative CTA findings are reliable in ruling out aneurysms in the PMH pattern or no blood on CT. DSA is indicated in the diffuse aneurysmal pattern of SAH, and repeat delayed DSA is required if the initial DSA findings are negative. When the blood is peripheral, CTA should be scrutinized for vasculitis and DSA is recommended for confirmation.
Figures
References
-
- Goddard AJ, Tan G, Becker J. Computed tomography angiography for the detection and characterization of intra-cranial aneurysms: current status. Clin Radiol 2005; 60: 1221–36 - PubMed
-
- Agid R, Lee SK, Willinsky RA, et al. . Acute subarachnoid hemorrhage: using 64-slice multidetector CT angiography to “triage” patients’ treatment. Neuroradiology 2006; 48: 787–94 - PubMed
-
- Willinsky RA, Taylor SM, TerBrugge K, et al. . Neurologic complications of cerebral angiography: prospective analysis of 2,899 procedures and review of the literature. Radiology 2003; 227: 522–28 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical