

Review
doi: 10.1016/j.clp.2009.08.001.
Neonatal seizures: an update on mechanisms and management
Affiliations
- PMID: 19944840
- PMCID: PMC2818833
- DOI: 10.1016/j.clp.2009.08.001
Item in Clipboard
Review
Neonatal seizures: an update on mechanisms and management
Clin Perinatol.
2009 Dec.
Abstract
The lifespan risk of seizures is highest in the neonatal period. Current therapies have limited efficacy. Although the treatment of neonatal seizures has not changed significantly in the last several decades, there has been substantial progress in understanding developmental mechanisms that influence seizure generation and responsiveness to anticonvulsants. This article provides an overview of current approaches to the diagnosis and treatment of neonatal seizures, and some of the recent insights about the pathophysiology of neonatal seizures that may provide the foundation for better treatment are identified.
Figures
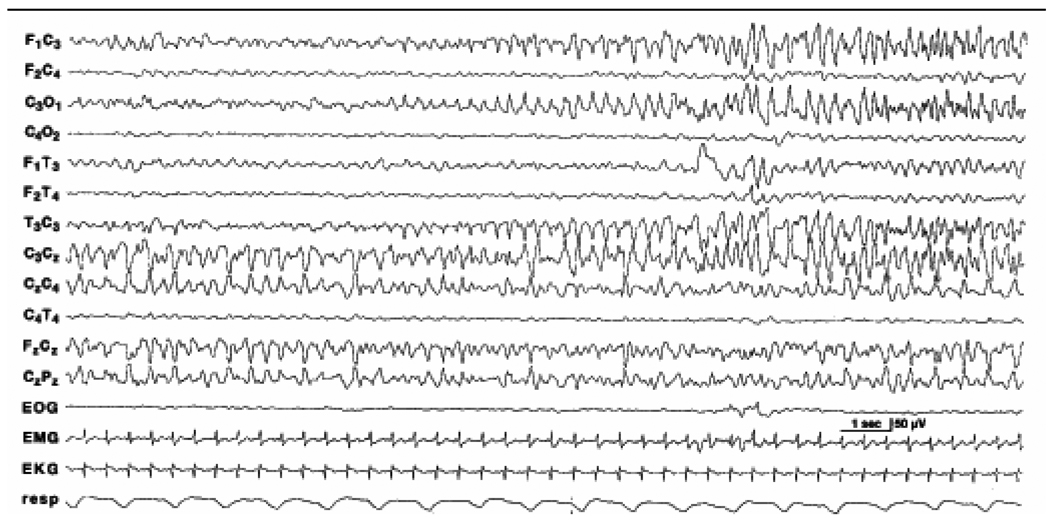
Electrical seizure activity begins in the midline central region (CZ) and then shifts to the left central region (C3). Toward the end of the seizures, as the electrical activity persists in the left central region, the midline central region becomes uninvolved. This electrical seizure activity occurred in the absence of any clinical seizure activity in this 40-week gestational age female infant with hypoxic-ischemic encephalopathy. She was initially comatose and hypotonic and, at the time of EEG recording, had been treated with phenobarbital. (Reprinted with permission from [136])
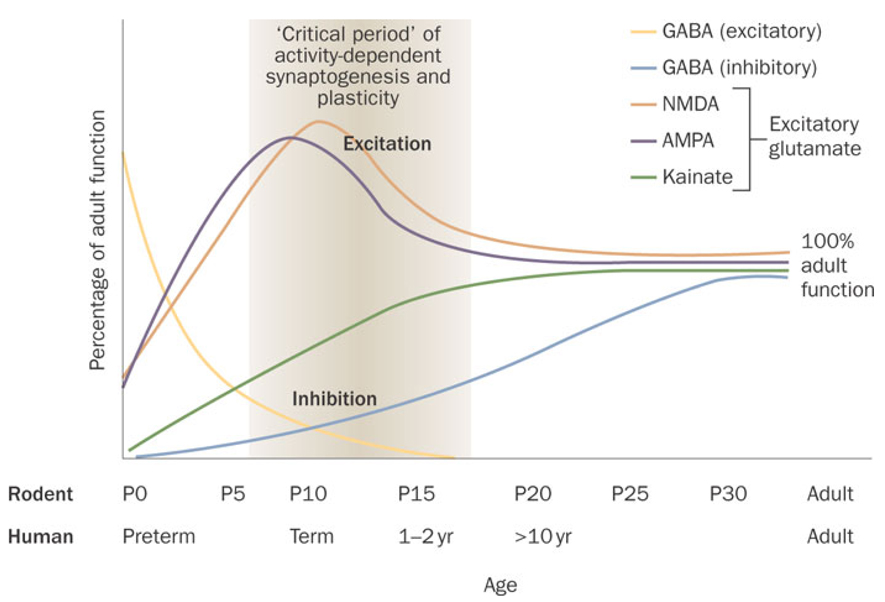
Equivalent developmental periods are displayed for rats and humans on the top and bottom x-axes, respectively. Activation of GABA receptors is depolarizing in rats early in the first postnatal week and in humans up to and including the neonatal period. Functional inhibition, however, is gradually reached over development in rats and humans. Prior to full maturation of GABA-mediated inhibition, the NMDA and AMPA subtypes of glutamate receptors peak between the first and second postnatal weeks in rats and in the neonatal period in humans. Kainate receptor binding is initially low and gradually rises to adult levels by the fourth postnatal week. Neonatal seizures emerge within the “critical period” of synaptogenesis and cerebral development. Abbreviations: AMPA, α-amino-3-hydroxy-5-methyl-4-isoxazole propionate; GABA, γ-aminobutyric acid; NMDA, N-methyl-D-aspartate; P, postnatal day. Reprinted from [45]. Permission obtained from Nature Reviews Neurology **.
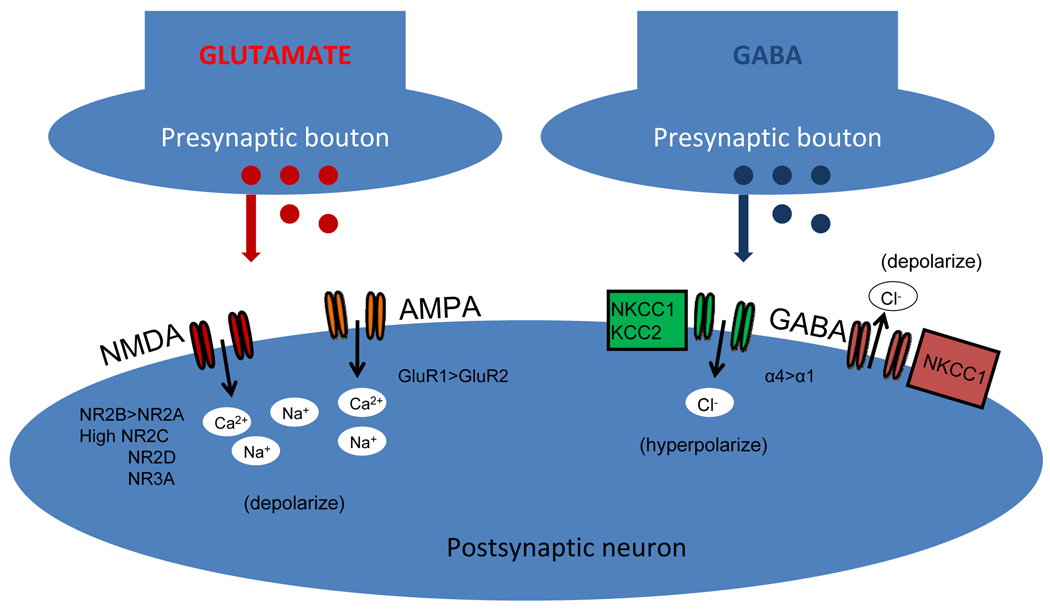
Depicted are an excitatory glutamatergic synapse (left panel) and a GABAergic inhibitory synapse (right panel). Presynaptic release of glutamate results in depolarization (excitation) of the postsynaptic neuron (left panel) by activation of NMDA and AMPA receptors. In contrast, release of GABA (right panel) results in hyperpolarization (inhibition) when the post synaptic neuron expresses sufficient quantities of the Cl− transporter KCC2, but depolarization (excitation) when intracellular Cl− accumulates due to unopposed action of the Cl− importer NKCC1. The immature glutamatergic receptors (left panel) are comprised of higher levels of NR2B, NR2C, NR2D, and NR3A subunits of the NMDA receptor, enhancing influx of Ca2+ and Na+ compared to mature synapses. In addition, AMPA receptors are relatively deficient in GluR2 subunits, resulting in relatively increased Ca2+ permeability compared to mature synapses. Hence specific NMDA receptor antagonists and AMPA receptor antagonists may prove to be age-specific therapeutic targets for treatment development. In addition, while GABAA receptor activation normally results in hyperpolarization and inhibition at mature synapses, due to the coexpression of NKCC1 and KCC2, the expression of KCC2 is low in the neonatal period compared with later in life and thus Cl− levels accumulate intracellularly and opening of GABAA receptors allows the passive efflux of Cl− out of the cell, resulting in paradoxical depolarization. In addition, GABAA receptor subunit expression in the immature brain is typified by higher levels of the α4 subunit, which is functionally associated with diminished benzodiazepine sensitivity. Both these attributes of the GABAA receptor make classical GABA agonists such as barbiturates and benzodiazepines less effective in the neonatal brain. The NKCC1 channel blocker bumetanide has anticonvulsant efficacy when administered with phenobarbital, suggesting a synergistic effect.
References
-
- Scher MS, Aso K, Beggarly ME, et al. Electrographic seizures in preterm and full-term neonates: clinical correlates, associated brain lesions, and risk for neurologic sequelae. Pediatrics. 1993;91:128–134. - PubMed
-
- Ronen GM, Penney S, Andrews W. The epidemiology of clinical neonatal seizures in Newfoundland: a population-based study. J.Pediatr. 1999;134(1):71–75. - PubMed
-
- Saliba RM, Annegers JF, Waller DK, et al. Incidence of neonatal seizures in Harris County, Texas, 1992–1994. Am.J Epidemiol. 1999;150(7):763–769. - PubMed
-
- Tekgul H, Gauvreau K, Soul J, et al. The current etiologic profile and neurodevelopmental outcome of seizures in term newborn infants. Pediatrics. 2006;117:1270–1280. - PubMed
-
- Volpe JJ. Neurology of the newborn. 5th edition. Philadelphia: Saunders/Elsevier; 2008.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
