

Clinical applications of a peptide-based vaccine for glioblastoma
- PMID: 19944970
- PMCID: PMC2824535
- DOI: 10.1016/j.nec.2009.09.001
Clinical applications of a peptide-based vaccine for glioblastoma
Abstract
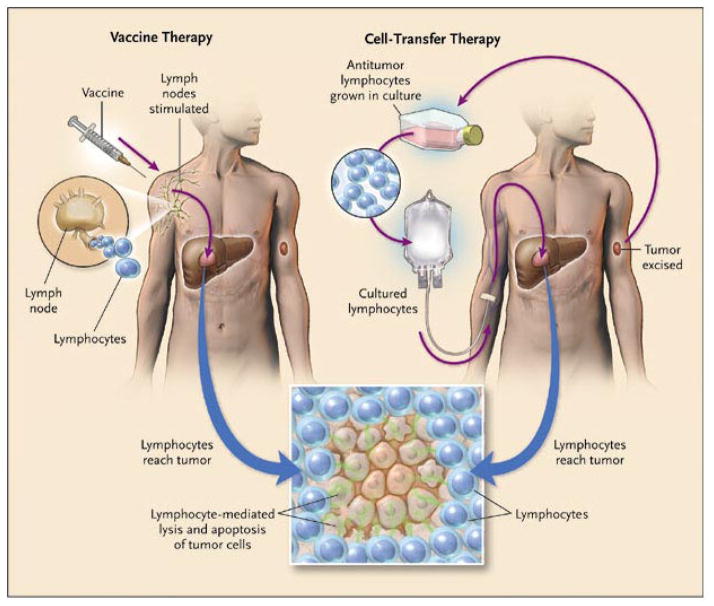
Glioblastoma multiforme is a malignant, relentless brain cancer with no known cure, and standard therapies leave significant room for the development of better, more effective treatments. Immunotherapy is a promising approach to the treatment of solid tumors that directs the patient's own immune system to destroy tumor cells. The most successful immunologically based cancer therapy to date involves the passive administration of monoclonal antibodies, but significant antitumor responses have also been generated with active vaccination strategies and cell-transfer therapies. This article summarizes the important components of the immune system, discusses the specific difficulty of immunologic privilege in the central nervous system, and reviews treatment approaches that are being attempted, with an emphasis on active immunotherapy using peptide vaccines.
Figures
References
-
- CBTRUS. Statistical Report: Primary Brain Tumors in the United States, 2000–2004. 2008.
-
- Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005 Mar 10;352(10):987–996. - PubMed
-
- Mocellin S, Mandruzzato S, Bronte V, Lise M, Nitti D. Part I: Vaccines for solid tumours. Lancet Oncol. 2004 Nov;5(11):681–689. - PubMed
-
- Pejawar-Gaddy S, Finn OJ. Cancer vaccines: accomplishments and challenges. Crit Rev Oncol Hematol. 2008 Aug;67(2):93–102. - PubMed
-
- Rosenberg SA, Lotze MT, Muul LM, et al. Observations on the systemic administration of autologous lymphokine-activated killer cells and recombinant interleukin-2 to patients with metastatic cancer. N Engl J Med. 1985 Dec 5;313(23):1485–1492. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
