

Review
doi: 10.1016/j.hfc.2009.08.001.
Genomics of pulmonary arterial hypertension: implications for therapy
Affiliations
- PMID: 19945066
- PMCID: PMC2786817
- DOI: 10.1016/j.hfc.2009.08.001
Item in Clipboard
Review
Genomics of pulmonary arterial hypertension: implications for therapy
Heart Fail Clin.
2010 Jan.
Abstract
Pulmonary arterial hypertension (PAH) remains a vexing clinical disease with no cure. Despite advances and the discovery of a gene (BMPR2) associated with many of the hereditary forms of the disease, and some cases not previously known to be inherited, the reasons for mutations in this gene as a cause remain somewhat elusive. Clearly, a complex interplay exists between genetic alterations, environmental exposures (including infections), and disease development. This article addresses the advances in the genetics of PAH, including the identification of genetic etiologies and modulators, and the role of genetics in predicting disease progression and targeting therapeutics.
Figures
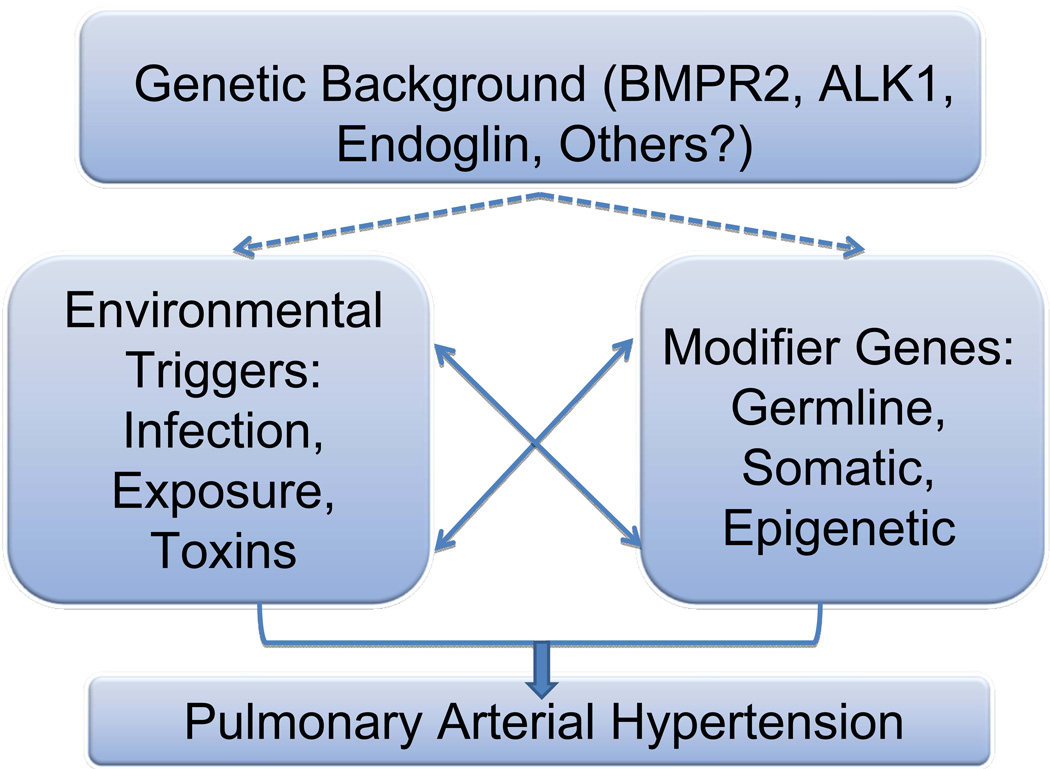
In this model, individuals may possess a genetic background that could predispose to the development of pulmonary hypertension. Since there is incomplete penetrance, even for heritable cases of PAH, other modifier events are highly likely to be causal, and can include environmental triggers such as exposures or infections, or the co-existence of modifier genes, either germline, somatic or epigenetic modifications. The interplay between genes and environment will undoubtedly prove extremely important in the definition of the etiology of the disease.
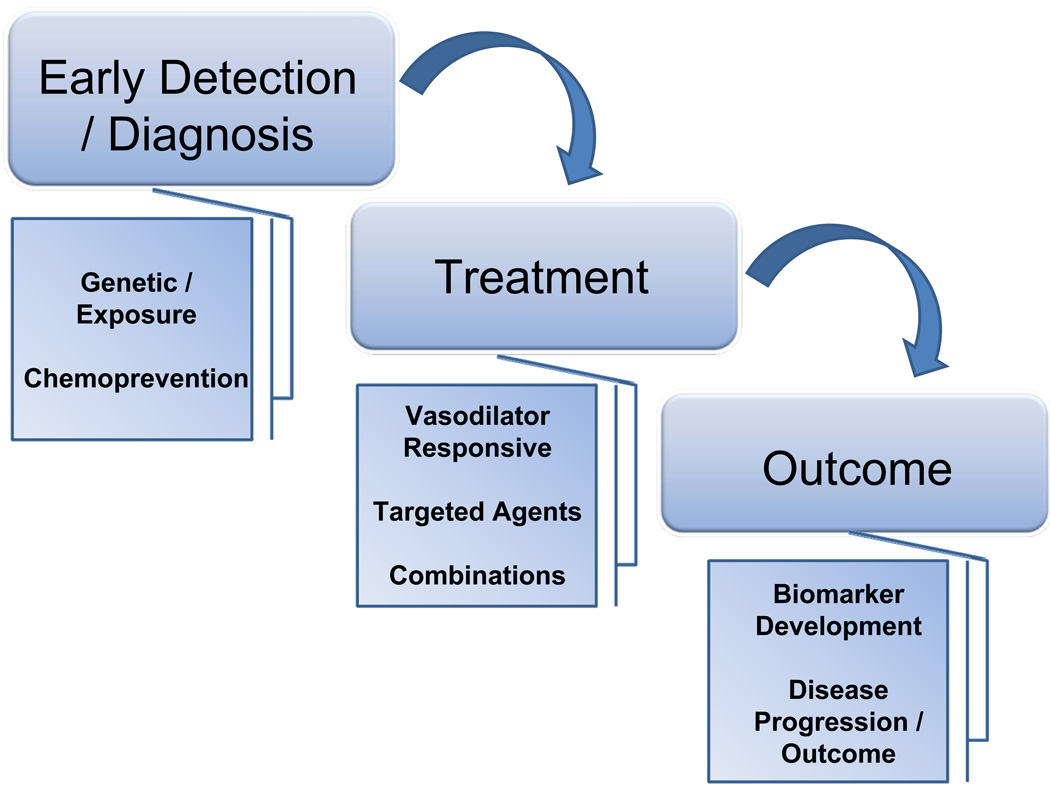
There are a number of exciting avenues for research. These follow along the continuum of diagnosis, treatment and outcome. Early diagnosis may lead to earlier interventions of treatment. Ultimately, with individuals at particularly high risk for disease development, chemoprevention strategies could be employed. Treatment will focus on new, targeted pathways based on novel pathway investigations. The hope of combinatorial treatments are emerging. The field is in dire need of biomarker development to follow, more accurately, disease progression.
Similar articles
-
Genetics and genomics of pulmonary arterial hypertension.J Am Coll Cardiol. 2013 Dec 24;62(25 Suppl):D13-21. doi: 10.1016/j.jacc.2013.10.035. J Am Coll Cardiol. 2013. PMID: 24355637 Review.
-
Genetic basis of pulmonary arterial hypertension: current understanding and future directions.J Am Coll Cardiol. 2004 Jun 16;43(12 Suppl S):33S-39S. doi: 10.1016/j.jacc.2004.02.028. J Am Coll Cardiol. 2004. PMID: 15194176 Review.
-
Genetic analyses in a cohort of 191 pulmonary arterial hypertension patients.Respir Res. 2018 May 9;19(1):87. doi: 10.1186/s12931-018-0789-9. Respir Res. 2018. PMID: 29743074 Free PMC article.
-
BMPR2 mutation alters the lung macrophage endothelin-1 cascade in a mouse model and patients with heritable pulmonary artery hypertension.Am J Physiol Lung Cell Mol Physiol. 2010 Sep;299(3):L363-73. doi: 10.1152/ajplung.00295.2009. Epub 2010 Jun 18. Am J Physiol Lung Cell Mol Physiol. 2010. PMID: 20562228 Free PMC article.
-
Cytoskeletal defects in Bmpr2-associated pulmonary arterial hypertension.Am J Physiol Lung Cell Mol Physiol. 2012 Mar 1;302(5):L474-84. doi: 10.1152/ajplung.00202.2011. Epub 2011 Dec 16. Am J Physiol Lung Cell Mol Physiol. 2012. PMID: 22180660 Free PMC article.
Cited by
-
Pulmonary arterial hypertension: are we close to the success?J Clin Respir Med. 2017;1(1):1-2. Epub 2017 Oct 12. J Clin Respir Med. 2017. PMID: 30740600 Free PMC article. No abstract available.
-
Early intervention in the management of pulmonary arterial hypertension: clinical and economic outcomes.Clinicoecon Outcomes Res. 2017 Nov 24;9:731-739. doi: 10.2147/CEOR.S119117. eCollection 2017. Clinicoecon Outcomes Res. 2017. PMID: 29200882 Free PMC article. Review.
-
Novel approaches to pulmonary arterial hypertension drug discovery.Expert Opin Drug Discov. 2016;11(4):407-14. doi: 10.1517/17460441.2016.1153625. Epub 2016 Feb 27. Expert Opin Drug Discov. 2016. PMID: 26901465 Free PMC article. Review.
-
Profile of Endothelin-1, Nitric Oxide, and Prostacyclin Levels in Pulmonary Arterial Hypertension Related to Uncorrected Atrial Septal Defect: Results from a Single Center Study in Indonesia.Cardiol Res Pract. 2020 Jan 7;2020:7526508. doi: 10.1155/2020/7526508. eCollection 2020. Cardiol Res Pract. 2020. PMID: 32377429 Free PMC article.
References
-
- Moncada S, Vane JR. Prostacyclin: its biosynthesis, actions and clinical potential. Philos Trans R Soc Lond B Biol Sci. 1981;294:305–329. - PubMed
-
- Cassin S, Tod ML, Frisinger JE, Jordan JA, Philips JB. Use of prostacyclin in persistent fetal circulation. Lancet. 1979;2:638. - PubMed
-
- Watkins WD, Peterson MB, Crone RK, Shannon DC, Levine L. Prostacyclin and prostaglandin E1 for severe idiopathic pulmonary artery hypertension. Lancet. 1980;1:1083. - PubMed
-
- Rubin LJ, Groves BM, Reeves JT, Frosolono M, Handel F, Cato AE. Prostacyclin-induced acute pulmonary vasodilation in primary pulmonary hypertension. Circulation. 1982;66:334–338. - PubMed
-
- Higenbottam T, Wheeldon D, Wells F, Wallwork J. Long-term treatment of primary pulmonary hypertension with continuous intravenous epoprostenol (prostacyclin) Lancet. 1984;1:1046–1047. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
