

Coronary perfusion pressure and return of spontaneous circulation after prolonged cardiac arrest
- PMID: 19947871
- PMCID: PMC2922866
- DOI: 10.3109/10903120903349796
Coronary perfusion pressure and return of spontaneous circulation after prolonged cardiac arrest
Abstract
Introduction: The amount of myocardial perfusion required for successful defibrillation after prolonged cardiac arrest is not known. Coronary perfusion pressure (CPP) is a surrogate for myocardial perfusion. One limited clinical study reported that a threshold of 15 mmHg was necessary for return of spontaneous circulation (ROSC), and that CPP was predictive of ROSC. A distinction between threshold and dose of CPP has not been reported.
Objective: To test the hypothesis that swine achieving ROSC will have higher preshock mean CPP and higher preshock area under the CPP curve (AUC) than swine not attaining ROSC.
Methods: Data from four similar swine cardiac arrest studies were retrospectively pooled. Animals had undergone 8-11 minutes of untreated ventricular fibrillation, 2 minutes of mechanical cardiopulmonary resuscitation (CPR), administration of drugs, and 3 more minutes of CPR prior to the first shock. Mean CPP +/- standard error of the mean (SEM) was derived from the last 20 compressions of each 30-second epoch of CPR and compared between ROSC/no-ROSC groups by repeated-measures analysis of variance (RM-ANOVA). AUC for all compressions delivered over the 5 minutes was calculated by direct summation and compared by Kruskal-Wallis test. Prediction of ROSC was assessed by logistic regression.
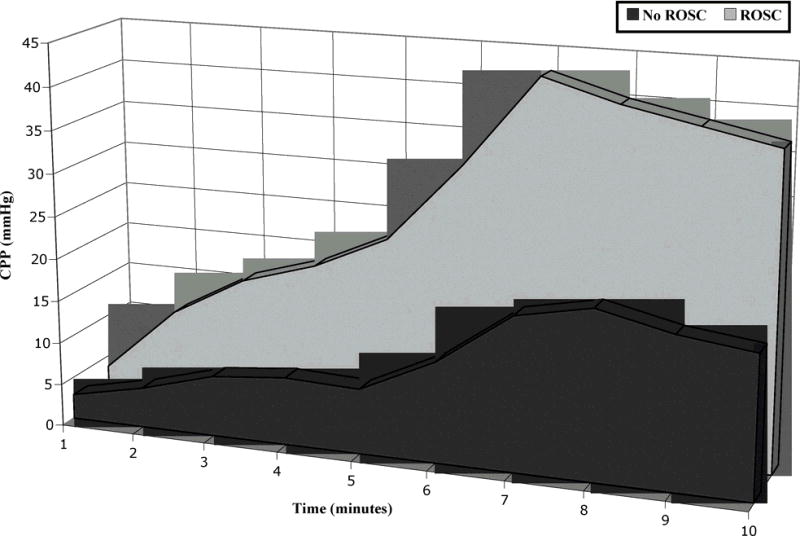
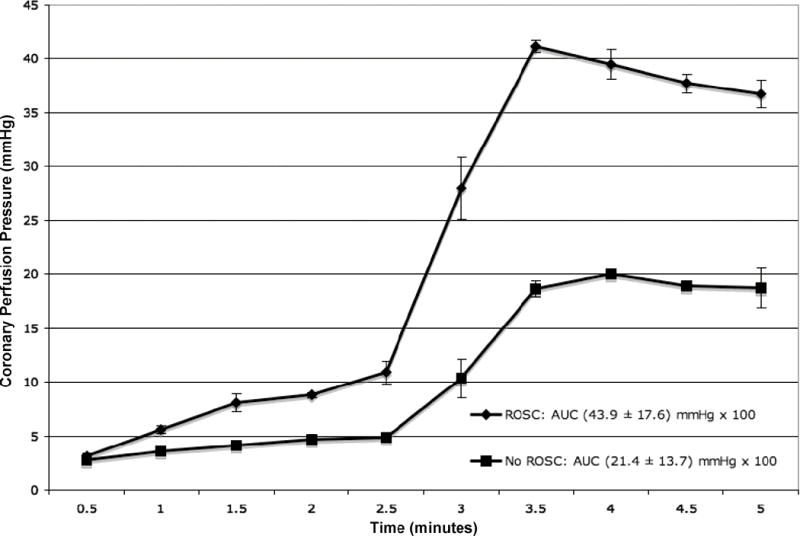
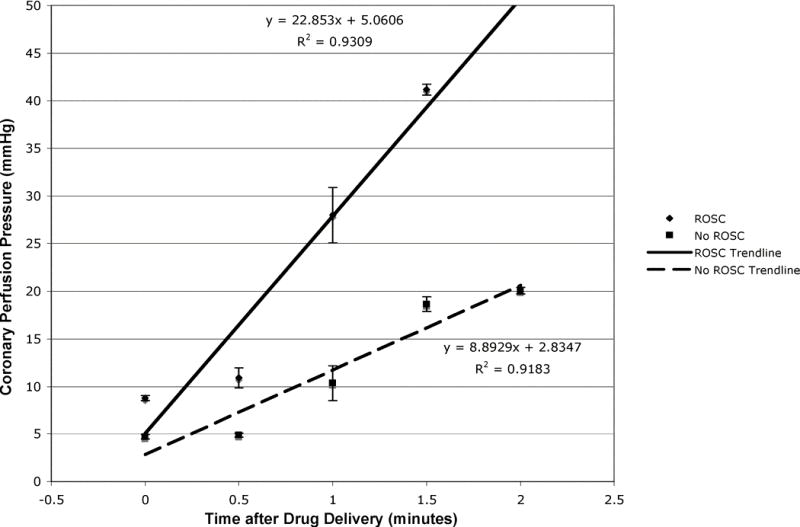
Results: Throughout the first 5 minutes of CPR (n = 80), mean CPP +/- SEM was consistently higher in animals with ROSC (n = 63) (maximum CPP 41.2 +/- 0.6 mmHg) than animals with no ROSC (maximum CPP 20.1 +/- 0.3 mmHg) (p = 0.0001). Animals with ROSC received more total reperfusion (43.9 +/- 17.6 mmHg x 10(2)) than animals without ROSC (21.4 +/- 13.7 mmHg x 10(2)) (p < 0.001). Two regression models identified CPP (odds ratio [OR] 1.11; 95% confidence interval [CI] 1.05, 1.18) and AUC (OR 1.10; 95% CI 1.05, 1.16) as predictors of ROSC. Experimental study also predicted ROSC in each model (OR 1.70; 95% CI 1.15, 2.50; and OR 1.59; 95% CI 1.12, 2.25, respectively).
Conclusion: Higher CPP threshold and dose are associated with and predictive of ROSC.
Figures
References
-
- Weisfeldt ML, Becker LB. Resuscitation after cardiac arrest: a 3-phase time-sensitive model. JAMA. 2002;288:3035–8. - PubMed
-
- Cobb LA, Fahrenbruch CE, Walsh TR, et al. Influence of cardiopulmonary resuscitation prior to defibrillation in patients with out-of-hospital ventricular fibrillation. JAMA. 1999;281:1182–8. - PubMed
-
- Wik L, Hansen TB, Fylling F, et al. Delaying defibrillation to give basic cardiopulmonary resuscitation to patients with out-of-hospital ventricular fibrillation: a randomized trial. JAMA. 2003;289:1389–95. - PubMed
-
- Berg RA, Hilwig RW, Ewy GA, Kern KB. Precountershock cardiopulmonary resuscitation improves initial response to defibrillation from prolonged ventricular fibrillation: a randomized, controlled swine study. Crit Care Med. 2004;32:1352–7. - PubMed
-
- Babbs CF. New versus old theories of blood flow during CPR. Crit Care Med. 1980;8:191–5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical