

Targeting the degradation of angiotensin II with recombinant angiotensin-converting enzyme 2: prevention of angiotensin II-dependent hypertension
- PMID: 19948988
- PMCID: PMC2827767
- DOI: 10.1161/HYPERTENSIONAHA.109.138420
Targeting the degradation of angiotensin II with recombinant angiotensin-converting enzyme 2: prevention of angiotensin II-dependent hypertension
Abstract
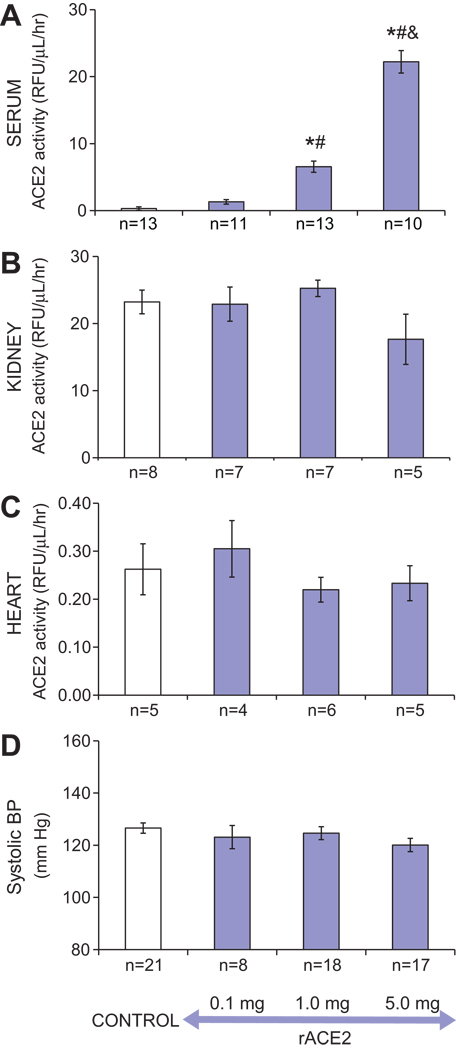
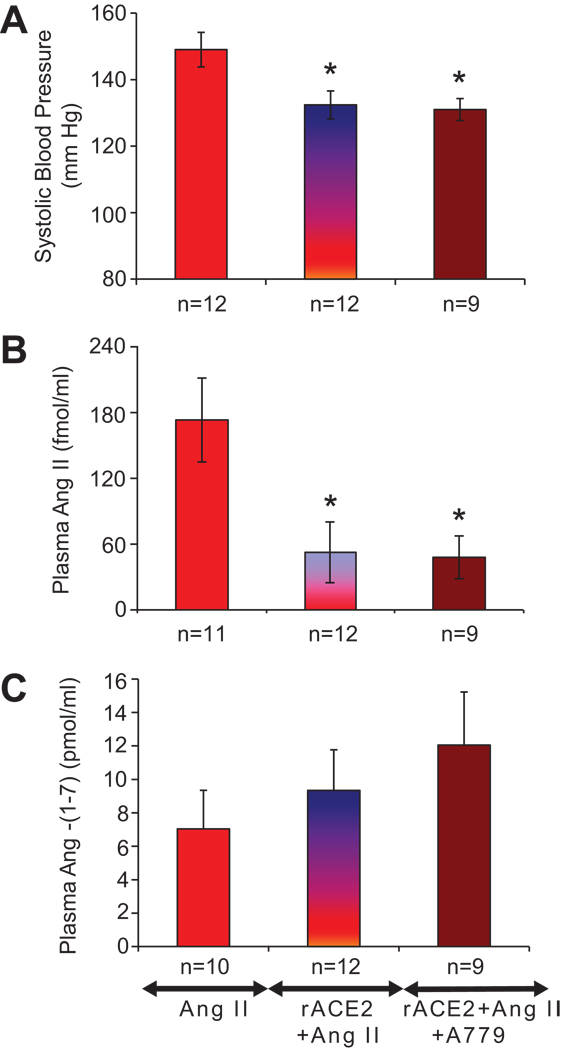
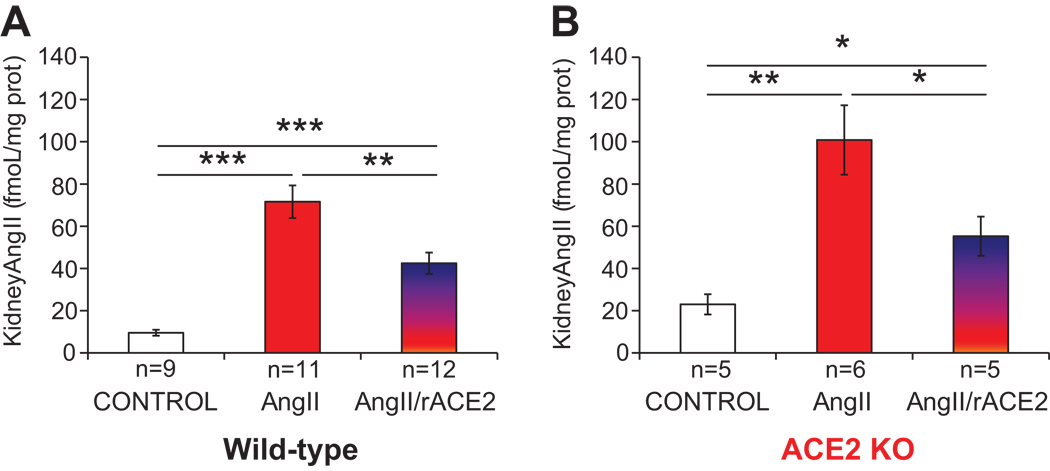
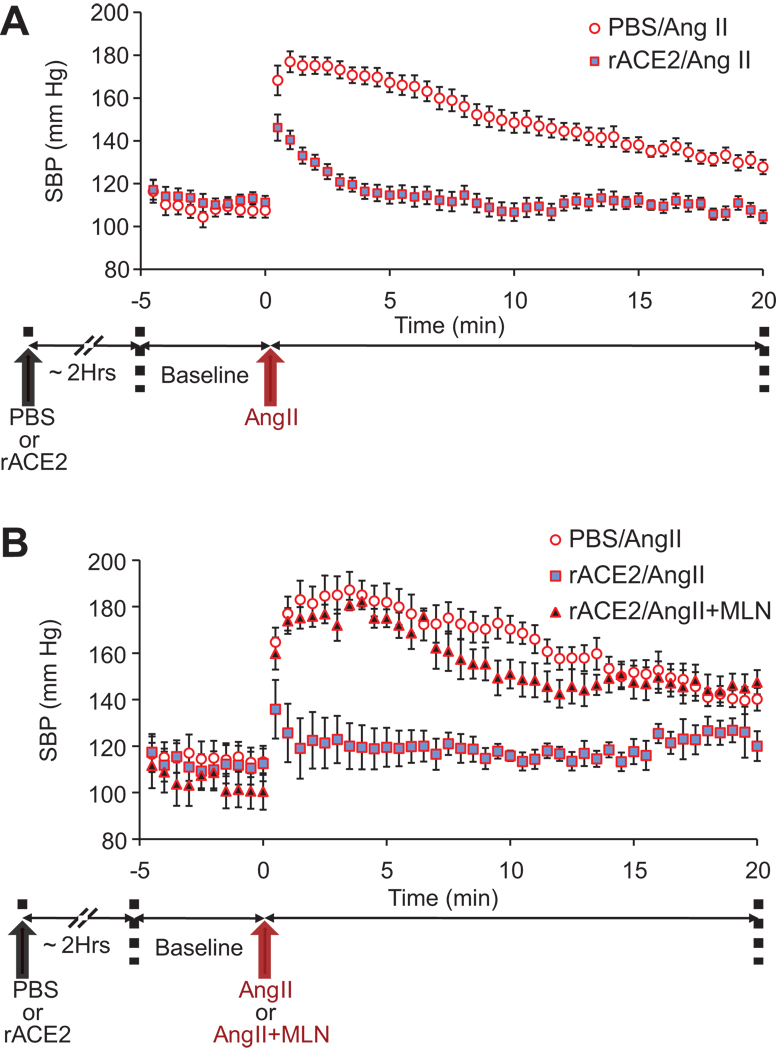
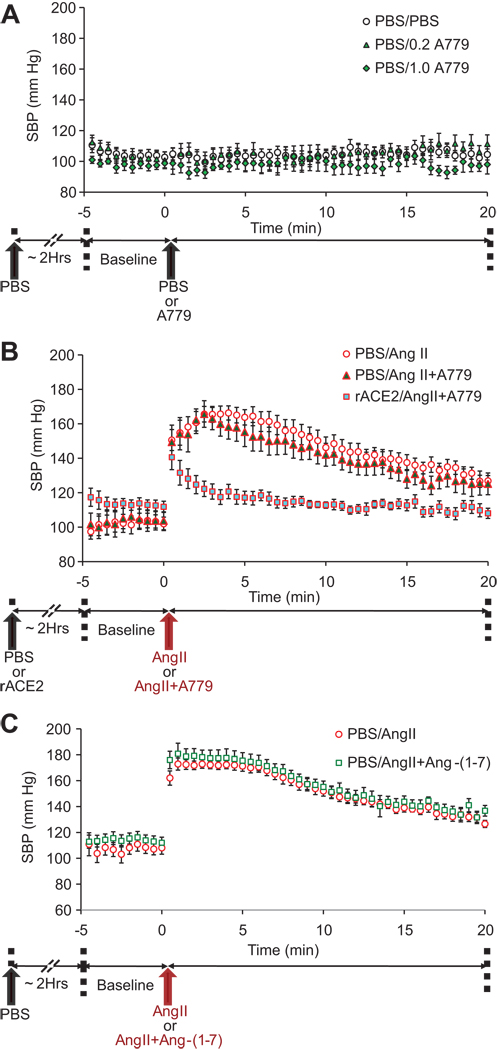
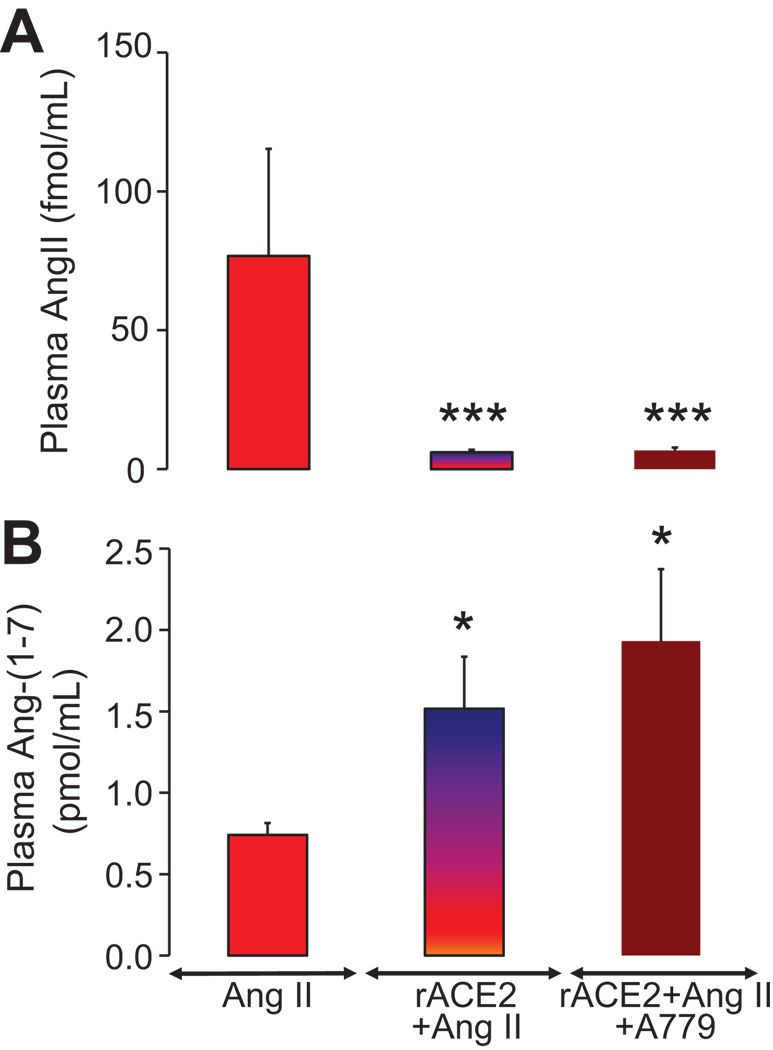
Angiotensin (Ang)-converting enzyme 2 (ACE2) cleaves Ang II to form Ang-(1-7). Here we examined whether soluble human recombinant ACE2 (rACE2) can efficiently lower Ang II and increase Ang-(1-7) and whether rACE2 can prevent hypertension caused by Ang II infusion as a result of systemic versus local mechanisms of ACE2 activity amplification. rACE2 was infused via osmotic minipumps for 3 days in conscious mice or acutely in anesthetized mice. rACE2 caused a dose-dependent increase in serum ACE2 activity but had no effect on kidney or cardiac ACE2 activity. After Ang II infusion (40 pmol/min), rACE2 (1 mg/kg per day) resulted in normalization of systolic blood pressure and plasma Ang II. In acute studies, rACE2 (1 mg/kg) prevented the rapid hypertensive effect of Ang II (0.2 mg/kg), and this was associated with both a decrease in Ang II and an increase in Ang-(1-7) in plasma. Moreover, during infusion of Ang II, the effect of rACE2 on blood pressure was unaffected by a specific Ang-(1-7) receptor blocker, A779 (0.2 mg/kg), and infusing supraphysiologic levels of Ang-(1-7) (0.2 mg/kg) had no effect on blood pressure. We conclude that, during Ang II infusion, rACE2 effectively degrades Ang II and, in the process, normalizes blood pressure. The mechanism of rACE2 action results from an increase in systemic, not tissue, ACE2 activity and the lowering of plasma Ang II rather than the attendant increase in Ang-(1-7). Increasing ACE2 activity may provide a new therapeutic target in states of Ang II overactivity by enhancing its degradation, an approach that differs from the current focus on blocking Ang II formation and action.
Figures
References
-
- Donoghue M, Hsieh F, Baronas E, Godbout K, Gosselin M, Stagliano N, Donovan M, Woolf B, Robison K, Jeyaseelan R, Breibart RE, Acton S. A novel angiotensin-coverting enzyme-related carboxypeptidase (ACE2) converts antiogensin I to angiotensin 1-9. Circ Res. 2000;87:E1–E9. - PubMed
-
- Tipnis SR, Hooper NM, Hyde R, Karran E, Christie G, Turner AJ. A human homolog of angiotensin-converting enzyme. Cloning and functional expression as a captopril-insensitive carboxypeptidase. J Biol Chem. 2000;274:33238–33243. - PubMed
-
- Vickers C, Hales P, Kaushik V, Dick L, Gavin J, Tang J, Godbout K, Parsons T, Baronas E, Hsieh F, Acton S, Patane M, Nichols A, Tummino P. Hydrolysis of biological peptides by human angiotensin-converting enzyme-related carboxypeptidase. J Biol Chem. 2002;277:14838–14843. - PubMed
-
- Ye M, Wysocki J, Naaz P, Salabat R, LaPointe MS, Batlle D. Increased ACE2 and decreased ACE protein in renal tubules from diabetic mice: A renoprotective combination? Hypertension. 2004;43:1120–1125. - PubMed
-
- Ye M, Wysocki J, William J, Soler MJ, Cokic I, Batlle D. Glomerular localization and expression of angiotensin-converting enzyme 2 and angiotensin-converting enzyme: implications for albuminuria in diabetes. J Am Soc Nephrol. 2006;17:3067–3075. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
