

Revised TN categorization for colon cancer based on national survival outcomes data
- PMID: 19949014
- PMCID: PMC2815715
- DOI: 10.1200/JCO.2009.24.0952
Revised TN categorization for colon cancer based on national survival outcomes data
Abstract
Purpose: The sixth edition of American Joint Committee on Cancer (AJCC) Cancer Staging Manual for colon cancer subdivided stage II into IIA (T3N0) and IIB (T4N0) and stage III into IIIA (T1-2N1M0), IIIB (T3-4N1M0), and IIIC (anyTN2M0). Subsequent analyses supported revised substaging of stage III because of improved survival for T1-2N2 versus T3-4N2 and T4N1 survival was more similar to T3-4N2 than to T3N1. The AJCC Hindgut Taskforce sought population-based validation that depth of invasion and nodal status interact to affect survival.
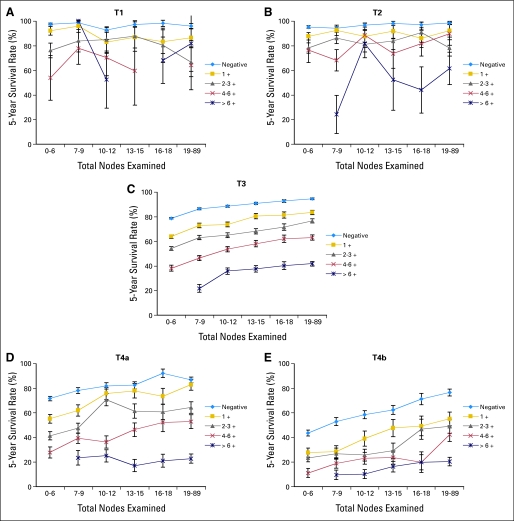
Patients and methods: Surveillance, Epidemiology, and End Results (SEER) population-based data from January 1992 to December 2004 for 109,953 colon cancer patients were compared with National Cancer Data Base (NCDB) data on 134,206 patients. T4N0 cancers were stratified by tumors that perforate visceral peritoneum (T4a) versus tumors that invade or are adherent to adjacent organs or structures (T4b). N1 and N2 were stratified by number of involved positive lymph nodes (N+): N1a/N1b (1 v 2-3), N2a/N2b (4 to 6 v > or = 7). Five-year observed and relative survival data were obtained for each TN category.
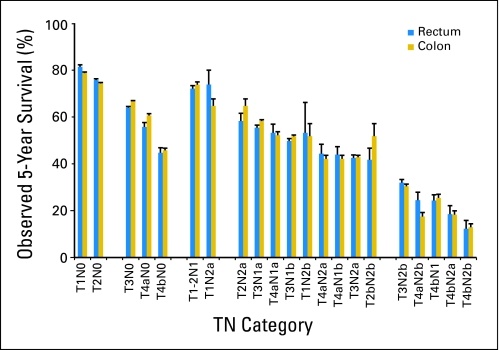
Results: SEER rectal cancer analyses confirm that T1-2N2 cancers have better prognosis than T3-4N2,T4bN1 have similar prognosis to T4N2, T1-2N1 have similar prognosis to T2N0/T3N0, and T1-2N2ahave similar prognosis to T2N0/T3N0 (T1N2a) or T4aN0 (T2N2a). Prognosis for T4a lesions is betterthan T4b by N category. The number of positive nodes affects prognosis.
Conclusion: This SEER population-based colon cancer analysis is highly consistent with rectal cancer pooled analysis and SEER rectal cancer analyses, supporting the shift of T1-2N2 lesions from IIIC to IIIA/IIIB, shifting T4bN1 from IIIB to IIIC, subdividing T4/N1/N2, and revising substaging of stages II/III. Survival outcomes by TN category for colon and rectal cancer are strikingly similar.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Revised staging: is it really better, or do we not know?J Clin Oncol. 2010 Aug 10;28(23):e397-8; author reply e399-400. doi: 10.1200/JCO.2010.28.5726. Epub 2010 Jun 14. J Clin Oncol. 2010. PMID: 20547986 No abstract available.
-
Conflicting finding on intramucosal colon cancers based on national survival outcomes data.J Clin Oncol. 2010 Sep 20;28(27):e469; author reply e470. doi: 10.1200/JCO.2010.29.2433. Epub 2010 Jun 28. J Clin Oncol. 2010. PMID: 20585093 No abstract available.
References
-
- Dukes CE. Cancer of the rectum: An analysis of 1000 cases. J Pathol. 1940;50:527–539.
-
- Copeland EM, Miller LD, Jones RS. Prognostic factors in carcinoma of the colon and rectum. Am J Surg. 1968;116:875–881. - PubMed
-
- Gunderson LL, Sosin H. Adenocarcinoma of the rectum: Areas of failure found at reoperation (second or symptomatic look) following curative surgery for adenocarcinoma of the rectum: Clinicopathologic correlation and implications for adjuvant therapy. Cancer. 1974;34:1278–1292. - PubMed
-
- Cass AW, Million RR, Pfaff WW. Patterns of recurrence following surgery alone for adenocarcinoma of the colon and rectum. Cancer. 1976;37:2861–2865. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
