

Truly "rational" polytherapy: maximizing efficacy and minimizing drug interactions, drug load, and adverse effects
- PMID: 19949567
- PMCID: PMC2730011
- DOI: 10.2174/157015909788848929
Truly "rational" polytherapy: maximizing efficacy and minimizing drug interactions, drug load, and adverse effects
Abstract
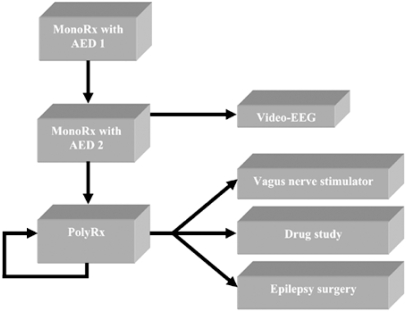
While several newer AEDs have study data that support monotherapy usage, most possess FDA indications for adjunctive treatment of partial onset seizures, leading to their initial (and often persistent) clinical use as adjunctive polytherapy for patients with refractory epilepsy. This review considers a practical approach to the appropriate role for polytherapy in epilepsy, presents the evidence for AED polytherapy, reviews the mythic but practically reasonable concept of "rational polytherapy," and concludes with practical strategies for avoiding and employing polytherapy in clinical practice. The appropriate indications for AED polytherapy include transitional polytherapy during titration of a new adjunctive AED toward monotherapy or long-term maintenance AED polytherapy in medically refractory epilepsy.
Keywords: Epilepsy; antiepileptic drugs; drug interactions.; drug load; polytherapy.
Figures
References
-
- Arroyo S, De La Morena A. Life-threatening adverse effects of antiepileptic drugs. Epilepsy Res. 2001;47:155–174. - PubMed
-
- Baulac M. Rational conversion from antiepileptic polytherapy to monotherapy. Epileptic Disord. 2003;5:125–132. - PubMed
-
- Bien CG, Kurthen M, Baron K, Lux S, Helmstaedter C, Schramm J, Elger CE. Long-term seizure outcome and antiepileptic drug treatment in surgically treated temporal lobe epilepsy patients: a controlled study. Epilepsia. 2001;42:1416–1421. - PubMed
-
- Boon P, D’Have M, Van Walleghem P, Michielsen G, Vonch K, Caemaert J, DeReuck J. Direct medical costs of refractory epilepsy incurred by three different treatment modalities: a prospective assessment. Epilepsia. 2002;43:96–102. - PubMed
-
- Bourgeois BF. Antiepileptic drug combinations and experimental background: the case of phenobarbital and phenytoin. Naunyn Schmiedebergs. Arch. Pharmacol. 1986;333:406–411. - PubMed
LinkOut - more resources
Full Text Sources