

A case of coronary artery dissection after aortic replacement in acute type a aortic dissection
- PMID: 19949589
- PMCID: PMC2771796
- DOI: 10.4070/kcj.2009.39.10.428
A case of coronary artery dissection after aortic replacement in acute type a aortic dissection
Abstract
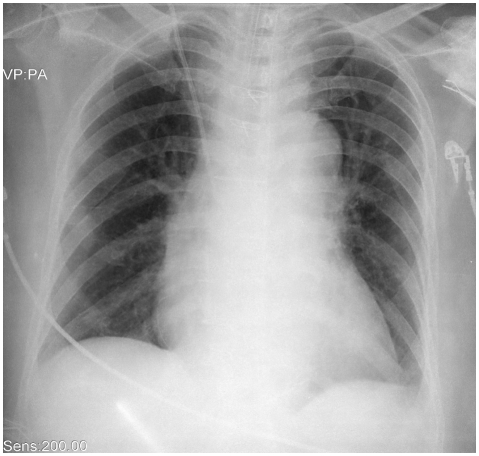
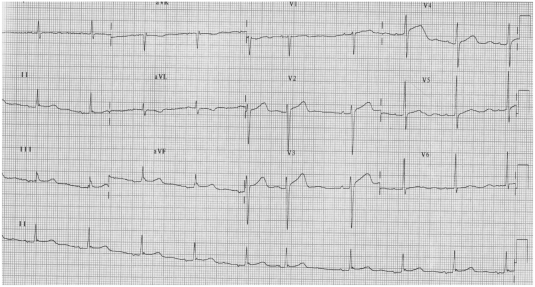
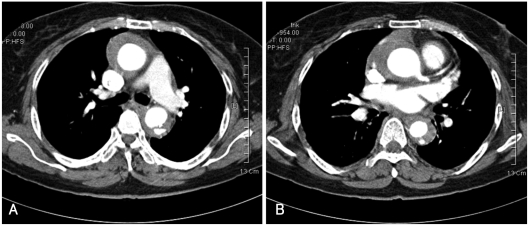
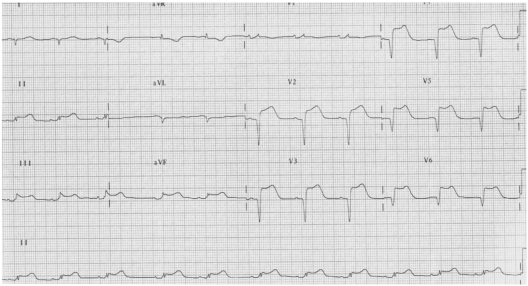
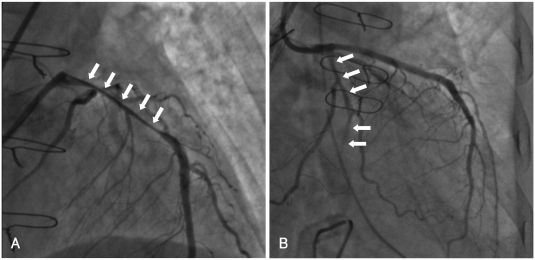
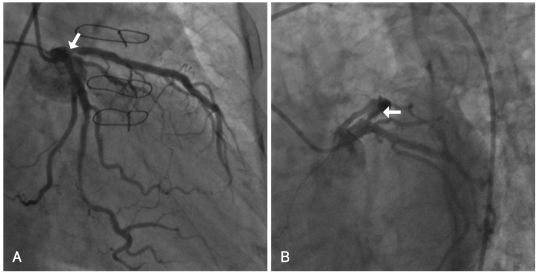
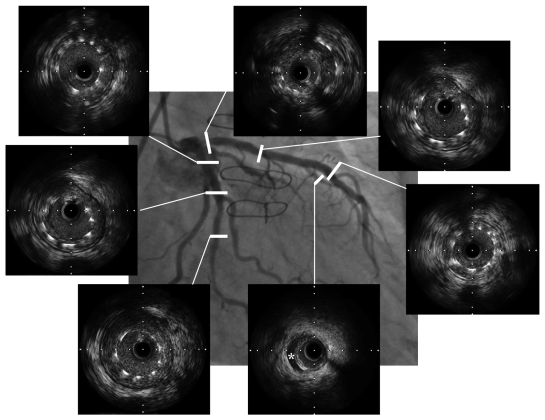
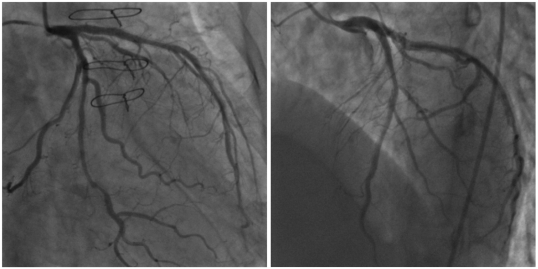
A 59-year-old woman was transferred to our institution with a diagnosis of acute type A aortic dissection. During aortic replacement surgery, the dissection had not extended to the orifice of the left coronary artery. However, ST segment elevation was observed on an electrocardiogram monitor immediately postoperatively. An emergent coronary angiogram showed almost complete collapse of the lumen of the left coronary artery due to pulsatile compression of the false lumen, which was caused by extension of the aortic dissection. Percutaneous coronary intervention (PCI) was performed with placement of stents in the left anterior descending artery (LAD) and left circumflex artery. Coronary angiography and intravascular ultrasound performed 45-days after PCI showed significant instent restenosis (ISR) at the proximal portion of the LAD and residual coronary artery dissection of the diagonal branch. Repeat balloon angioplasty was performed at the site of the ISR. A follow-up coronary angiogram 8-months after the PCI showed no evidence of ISR.
Keywords: Aortic diseases; Cordiovascalar surgical procedures; Myocardial infarction; Percutaneous transluminal coronary angioplasty.
Figures
Similar articles
-
Intravascular ultrasound-guided percutaneous coronary intervention for total occlusion of the proximal left anterior descending artery caused by spontaneous coronary dissection in a young woman.Cardiovasc Interv Ther. 2012 Jan;27(1):31-5. doi: 10.1007/s12928-011-0076-x. Epub 2011 Jul 26. Cardiovasc Interv Ther. 2012. PMID: 24122638 Review.
-
The Young Heart Tears Easily Apart: A Case Report of Spontaneous Coronary Artery Dissection.Cureus. 2021 Jun 11;13(6):e15590. doi: 10.7759/cureus.15590. eCollection 2021 Jun. Cureus. 2021. PMID: 34277211 Free PMC article.
-
Iatrogenic propagation of left main coronary artery dissection during diagnostic coronary angiography: A case report.Medicine (Baltimore). 2025 Apr 4;104(14):e42040. doi: 10.1097/MD.0000000000042040. Medicine (Baltimore). 2025. PMID: 40193674 Free PMC article.
-
Progression of left coronary artery dissection during and after aortic replacement in acute type A aortic dissection: a case report.Ann Thorac Cardiovasc Surg. 2007 Jun;13(3):209-12. Ann Thorac Cardiovasc Surg. 2007. PMID: 17592433
-
Spontaneous retrograde dissection of ascending aorta from descending thoracic aorta--a case review.Perfusion. 2011 May;26(3):215-22. doi: 10.1177/0267659110395804. Epub 2011 Jan 19. Perfusion. 2011. PMID: 21247986 Review.
Cited by
-
Aortic dissection and rupture in an 11-year-old child: A case report.J Cardiol Cases. 2010 Oct 15;3(1):e46-e49. doi: 10.1016/j.jccase.2010.08.001. eCollection 2011 Feb. J Cardiol Cases. 2010. PMID: 30532834 Free PMC article.
-
A case of spontaneous coronary artery dissection healed by medical treatment: serial findings of coronary angiography, intravascular ultrasound and multi-detector computed tomography.Korean Circ J. 2011 Jun;41(6):346-8. doi: 10.4070/kcj.2011.41.6.346. Epub 2011 Jun 30. Korean Circ J. 2011. PMID: 21779291 Free PMC article.
-
Aortic dissection and rupture in a child.Korean Circ J. 2011 Mar;41(3):156-9. doi: 10.4070/kcj.2011.41.3.156. Epub 2011 Mar 31. Korean Circ J. 2011. Retraction in: Korean Circ J. 2012 Jul;42(7):511. doi: 10.4070/kcj.2012.42.7.511. PMID: 21519516 Free PMC article. Retracted.
References
-
- Nah DY, Park KU, Kim SH. Acute proximal aortic dissection associated with ST segment elevation on electrocardiography. Korean Circ J. 2004;34:795–798.
-
- Kawahito K, Adachi H, Murata S, Yamaguchi A, Ino T. Coronary malperfusion due to type A aortic dissection: mechanism and surgical management. Ann Thorac Surg. 2003;76:1471–1476. - PubMed
-
- Neri E, Toscano T, Papalia U, et al. Proximal aortic dissection with coronary malperfusion: presentation, management, and outcome. J Thorac Cardiovasc Surg. 2001;121:552–560. - PubMed
-
- Kwon YS, Lee HS, Shin JK, et al. A case of left main coronary stenting for acute myocardial infarction complicated by ascending aortic dissection. Korean Circ J. 2004;34:1210–1215.
-
- Horszczaruk GJ, Roik MF, Kochman J, et al. Aortic dissection involving ostium of right coronary artery as the reason of myocardial infarction. Eur Heart J. 2006;27:518. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
