

Founder mutations in the Netherlands: SCN5a 1795insD, the first described arrhythmia overlap syndrome and one of the largest and best characterised families worldwide
- PMID: 19949711
- PMCID: PMC2779479
- DOI: 10.1007/BF03086296
Founder mutations in the Netherlands: SCN5a 1795insD, the first described arrhythmia overlap syndrome and one of the largest and best characterised families worldwide
Abstract
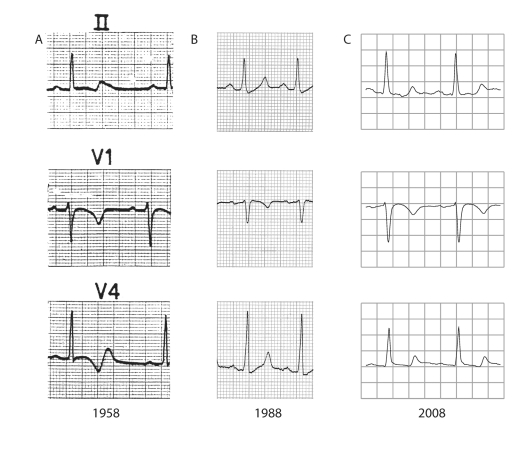
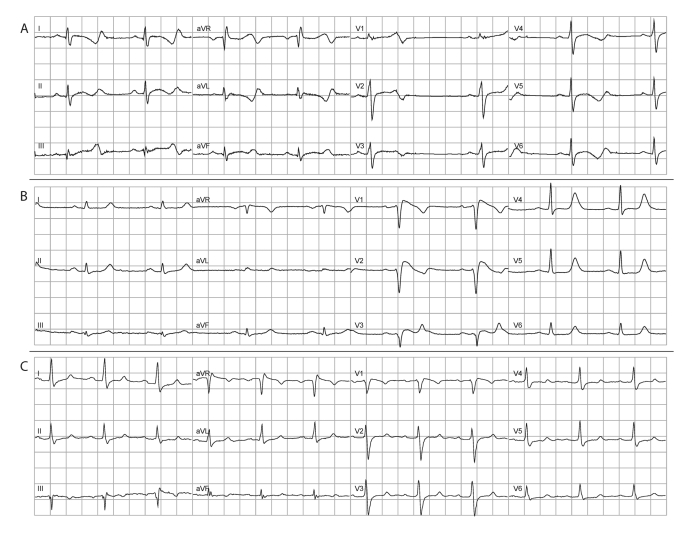
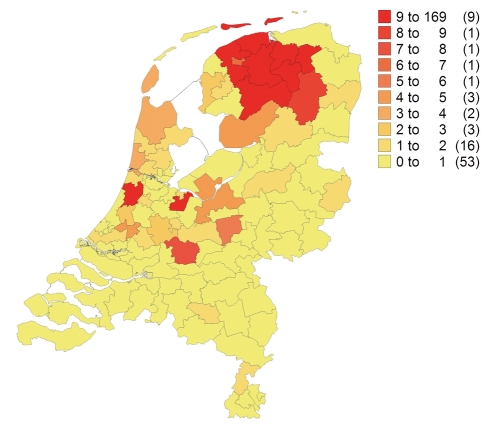
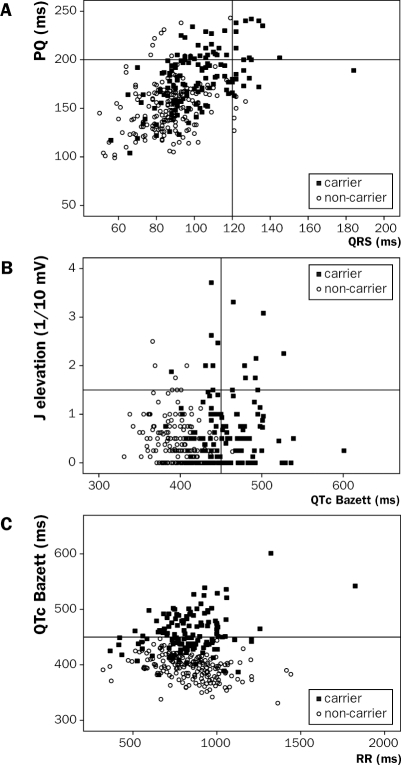
In this part of a series on founder mutations in the Netherlands, we review a Dutch family carrying the SCN5a 1795insD mutation. We describe the advances in our understanding of the premature sudden cardiac deaths that have accompanied this family in the past centuries. The mutation carriers show a unique overlap of long-QT syndrome (type 3), Brugada syndrome and progressive cardiac conduction defects attributed to a single mutation in the cardiac sodium channel gene SCN5a. It is at present one of the largest and best-described families worldwide and we have learned immensely from the mouse strains with the murine homologue of the SCN5a 1795insD mutation (SCN5a 1798insD). From the studies currently performed we are about to obtain new insights into the phenotypic variability in this monogenic arrhythmia syndrome, and this might also be relevant for other arrhythmia syndromes and the general population. (Neth Heart J 2009;17:422-8.).
Keywords: Brugada syndrome; cardiac sodium channel disease; conduction disease; long-QT syndrome; sudden cardiac death.
Figures
Similar articles
-
SCN5A-1795insD founder variant: a unique Dutch experience spanning 7 decades.Neth Heart J. 2023 Aug;31(7-8):263-271. doi: 10.1007/s12471-023-01799-8. Epub 2023 Jul 20. Neth Heart J. 2023. PMID: 37474841 Free PMC article. Review.
-
Overlap syndrome of cardiac sodium channel disease in mice carrying the equivalent mutation of human SCN5A-1795insD.Circulation. 2006 Dec 12;114(24):2584-94. doi: 10.1161/CIRCULATIONAHA.106.653949. Epub 2006 Dec 4. Circulation. 2006. PMID: 17145985
-
Heritability in a SCN5A-mutation founder population with increased female susceptibility to non-nocturnal ventricular tachyarrhythmia and sudden cardiac death.Heart Rhythm. 2017 Dec;14(12):1873-1881. doi: 10.1016/j.hrthm.2017.07.036. Epub 2017 Aug 3. Heart Rhythm. 2017. PMID: 28782696
-
Gating-dependent mechanisms for flecainide action in SCN5A-linked arrhythmia syndromes.Circulation. 2001 Sep 4;104(10):1200-5. doi: 10.1161/hc3501.093797. Circulation. 2001. PMID: 11535580
-
Clinical Spectrum of SCN5A Mutations: Long QT Syndrome, Brugada Syndrome, and Cardiomyopathy.JACC Clin Electrophysiol. 2018 May;4(5):569-579. doi: 10.1016/j.jacep.2018.03.006. Epub 2018 May 2. JACC Clin Electrophysiol. 2018. PMID: 29798782 Review.
Cited by
-
Recurrent and Founder Mutations in the Netherlands: the Long-QT Syndrome.Neth Heart J. 2011 Jan;19(1):10-16. doi: 10.1007/s12471-010-0046-4. Epub 2010 Dec 17. Neth Heart J. 2011. PMID: 21350584 Free PMC article.
-
Inherited cardiac arrhythmias.Nat Rev Dis Primers. 2020 Jul 16;6(1):58. doi: 10.1038/s41572-020-0188-7. Nat Rev Dis Primers. 2020. PMID: 32678103 Free PMC article. Review.
-
Cardiac ion channelopathies and the sudden infant death syndrome.ISRN Cardiol. 2012;2012:846171. doi: 10.5402/2012/846171. Epub 2012 Dec 5. ISRN Cardiol. 2012. PMID: 23304551 Free PMC article.
-
Founder mutations in the Netherlands: familial idiopathic ventricular fibrillation and DPP6.Neth Heart J. 2011 Jun;19(6):290-6. doi: 10.1007/s12471-011-0102-8. Neth Heart J. 2011. PMID: 21512816 Free PMC article.
-
Genetic background determines the severity of age-dependent cardiac structural abnormalities and arrhythmia susceptibility in Scn5a-1798insD mice.Europace. 2024 Jun 3;26(6):euae153. doi: 10.1093/europace/euae153. Europace. 2024. PMID: 38875491 Free PMC article.
References
-
- Bezzina C, Veldkamp MW, van den Berg MP, Postma AV, Rook MB, Viersma JW, et al. A single Na(+) channel mutation causing both long-QT and Brugada syndromes. Circ Res. 1999;85:1206–13. - PubMed
-
- Veldkamp MW, Viswanathan PC, Bezzina C, Baartscheer A, Wilde AA, Balser JR. Two distinct congenital arrhythmias evoked by a multidysfunctional Na(+) channel. Circ Res. 2000;86:E91–E97. - PubMed
-
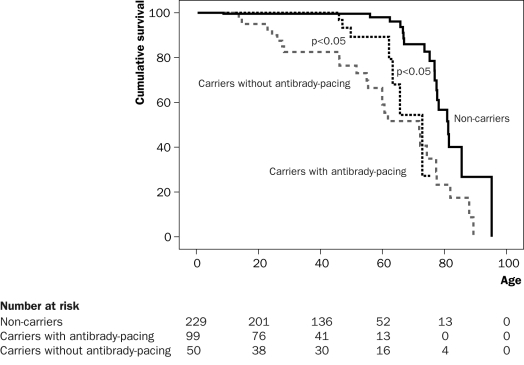
- van den Berg MP, Wilde AA, Viersma TJW, Brouwer J, Haaksma J, van der Hout AH, et al. Possible bradycardic mode of death and successful pacemaker treatment in a large family with features of long QT syndrome type 3 and Brugada syndrome. J Cardiovasc Electrophysiol. 2001;12:630–6. - PubMed
-
- Viswanathan PC, Bezzina CR, George AL Jr, Roden DM, Wilde AA, Balser JR. Gating-dependent mechanisms for flecainide action in SCN5A-linked arrhythmia syndromes. Circulation. 2001;104:1200–5. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous