

Assessment of tissue oxygen saturation during a vascular occlusion test using near-infrared spectroscopy: the role of probe spacing and measurement site studied in healthy volunteers
- PMID: 19951388
- PMCID: PMC2786106
- DOI: 10.1186/cc8002
Assessment of tissue oxygen saturation during a vascular occlusion test using near-infrared spectroscopy: the role of probe spacing and measurement site studied in healthy volunteers
Abstract
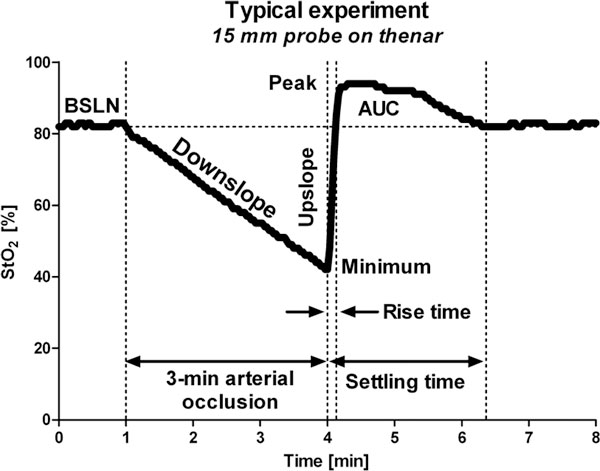
Introduction: To assess potential metabolic and microcirculatory alterations in critically ill patients, near-infrared spectroscopy (NIRS) has been used, in combination with a vascular occlusion test (VOT), for the non-invasive measurement of tissue oxygen saturation (StO2), oxygen consumption, and microvascular reperfusion and reactivity. The methodologies for assessing StO2 during a VOT, however, are very inconsistent in the literature and, consequently, results vary from study to study, making data comparison difficult and potentially inadequate. Two major aspects concerning the inconsistent methodology are measurement site and probe spacing. To address these issues, we investigated the effects of probe spacing and measurement site using 15 mm and 25 mm probe spacings on the thenar and the forearm in healthy volunteers and quantified baseline, ischemic, reperfusion, and hyperemic VOT-derived StO2 variables.
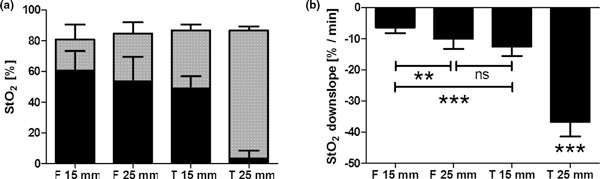
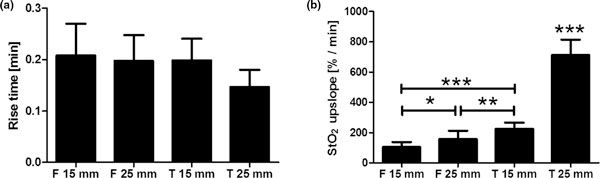
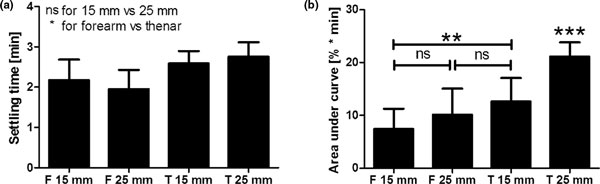
Methods: StO2 was non-invasively measured in the forearm and thenar in eight healthy volunteers during 3-minute VOTs using two InSpectra tissue spectrometers equipped with a 15 mm probe or a 25 mm probe. VOT-derived StO2 traces were analyzed for base-line, ischemic, reperfusion, and hyperemic parameters. Data were categorized into four groups: 15 mm probe on the forearm (F15 mm), 25 mm probe on the forearm (F25 mm), 15 mm probe on the thenar (T15 mm), and 25 mm probe on the thenar (T25 mm).
Results: Although not apparent at baseline, probe spacing and measurement site significantly influenced VOT-derived StO2 variables. For F15 mm, F25 mm, T15 mm, and T25 mm, StO2 ownslope was -6.4 +/- 1.7%/minute, -10.0 +/- 3.2%/minute, -12.5 +/- 3.0%/minute, and -36.7 +/- 4.6%/minute, respectively. StO2 upslope was 105 +/- 34%/minute, 158 +/- 55%/minute, 226 +/- 41%/minute, and 713 +/- 101%/minute, and the area under the hyperemic curve was 7.4 +/- 3.8%.minute, 10.1 +/- 4.9%.minute, 12.6 +/- 4.4%.minute, and 21.2 +/- 2.7%.minute in these groups, respectively. Furthermore, the StO2 parameters of the hyperemic phase of the VOT, such as the area under the curve, significantly correlated to the minimum StO2 during ischemia.
Conclusions: NIRS measurements in combination with a VOT are measurement site-dependent and probe-dependent. Whether this dependence is anatomy-, physiology-, or perhaps technology-related remains to be elucidated. Our study also indicated that reactive hyperemia depends on the extent of ischemic insult.
Figures
Similar articles
-
Characterization of tissue oxygen saturation and the vascular occlusion test: influence of measurement sites, probe sizes and deflation thresholds.Crit Care. 2009;13 Suppl 5(Suppl 5):S3. doi: 10.1186/cc8001. Epub 2009 Nov 30. Crit Care. 2009. PMID: 19951387 Free PMC article.
-
Near-infrared spectroscopy for assessing tissue oxygenation and microvascular reactivity in critically ill patients: a prospective observational study.Crit Care. 2016 Oct 1;20(1):311. doi: 10.1186/s13054-016-1500-5. Crit Care. 2016. PMID: 27716370 Free PMC article.
-
Simultaneous multi-depth assessment of tissue oxygen saturation in thenar and forearm using near-infrared spectroscopy during a simple cardiovascular challenge.Crit Care. 2009;13 Suppl 5(Suppl 5):S5. doi: 10.1186/cc8003. Epub 2009 Nov 30. Crit Care. 2009. PMID: 19951389 Free PMC article.
-
Resonance Raman Spectroscopy Tissue Oxygenation Measurements in Neonates.Neonatology. 2023;120(3):363-370. doi: 10.1159/000529624. Epub 2023 Mar 30. Neonatology. 2023. PMID: 36996764 Review.
-
Skeletal muscle oxygen saturation (StO2) measured by near-infrared spectroscopy in the critically ill patients.Biomed Res Int. 2013;2013:502194. doi: 10.1155/2013/502194. Epub 2013 Aug 21. Biomed Res Int. 2013. PMID: 24027757 Free PMC article. Review.
Cited by
-
No effect of fitness on brachial or forearm vascular function during acute inflammation in young adults.Am J Physiol Regul Integr Comp Physiol. 2019 Nov 1;317(5):R746-R753. doi: 10.1152/ajpregu.00120.2019. Epub 2019 Sep 25. Am J Physiol Regul Integr Comp Physiol. 2019. PMID: 31553624 Free PMC article.
-
Cross-section and feasibility study on the non-invasive evaluation of muscle hemodynamic responses in Duchenne muscular dystrophy by using a near-infrared diffuse optical technique.Biomed Opt Express. 2018 Sep 12;9(10):4767-4780. doi: 10.1364/BOE.9.004767. eCollection 2018 Oct 1. Biomed Opt Express. 2018. PMID: 30319901 Free PMC article.
-
Effects of high oxygen tension on healthy volunteer microcirculation.Diving Hyperb Med. 2022 Dec 20;52(4):260-70. doi: 10.28920/dhm52.4.260-270. Diving Hyperb Med. 2022. PMID: 36525683 Free PMC article.
-
Tissue saturation measurement--exciting prospects, but standardisation and reference data still needed.Crit Care. 2010;14(3):169. doi: 10.1186/cc8970. Epub 2010 Jun 24. Crit Care. 2010. PMID: 20619003 Free PMC article.
-
Tissue oxygen saturation changes and postoperative complications in cardiac surgery: a prospective observational study.BMC Anesthesiol. 2019 Dec 16;19(1):229. doi: 10.1186/s12871-019-0905-5. BMC Anesthesiol. 2019. PMID: 31842777 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
