

Validation of an algorithm for categorizing the severity of hospital emergency department visits
- PMID: 19952803
- PMCID: PMC3881233
- DOI: 10.1097/MLR.0b013e3181bd49ad
Validation of an algorithm for categorizing the severity of hospital emergency department visits
Abstract
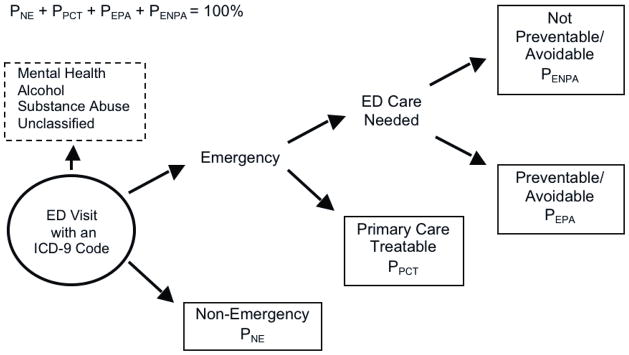
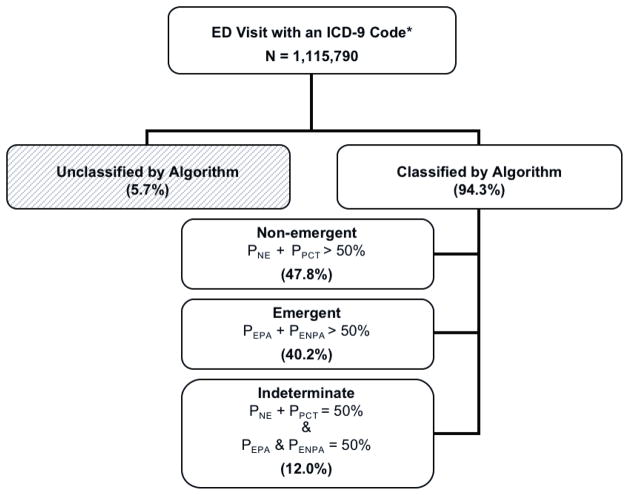
Background: Differentiating between appropriate and inappropriate resource use represents a critical challenge in health services research. The New York University Emergency Department (NYU ED) visit severity algorithm attempts to classify visits to the ED based on diagnosis, but it has not been formally validated.
Objective: To assess the validity of the NYU algorithm.
Research design: A longitudinal study in a single integrated delivery system from January 1999 to December 2001.
Subjects: A total of 2,257,445 commercial and 261,091 Medicare members of an integrated delivery system.
Measures: ED visits were classified as emergent, nonemergent, or intermediate severity, using the NYU ED algorithm. We examined the relationship between visit-severity and the probability of future hospitalizations and death using a logistic model with a general estimating equation approach.
Results: Among commercially insured subjects, ED visits categorized as emergent were significantly more likely to result in a hospitalization within 1-day (odds ratio = 3.37, 95% CI: 3.31-3.44) or death within 30-days (odds ratio = 2.81, 95% CI: 2.62-3.00) than visits categorized as nonemergent. We found similar results in Medicare patients and in sensitivity analyses using different probability thresholds. ED overuse for nonemergent conditions was not related to socio-economic status or insurance type.
Conclusions: The evidence presented supports the validity of the NYU ED visit severity algorithm for differentiating ED visits based on need for hospitalization and/or mortality risk; therefore, it can contribute to evidence-based policies aimed at reducing the use of the ED for nonemergencies.
Figures
Comment in
-
Comment on Ballard DW, Price M, Fung V, et al. Validation of an algorithm for categorizing the severity of hospital emergency department visits. Med Care. 2010;48(1):58-63.Med Care. 2010 May;48(5):395. doi: 10.1097/MLR.0b013e3181db53b7. Med Care. 2010. PMID: 20393358 No abstract available.
-
Comment on Ballard DW, Price M, Fung V, et al. Validation of an algorithm for categorizing the severity of hospital emergency department visits. Med Care. 2010; 48(1): 58-63.Med Care. 2012 Apr;50(4):361; author reply 361-2. doi: 10.1097/MLR.0b013e3181db53b7. Med Care. 2012. PMID: 22411442 No abstract available.
References
-
- Institute of Medicine. Hospital-Based Emergency Care: At the Breaking Point. Washington, DC: National Academy Press; 2006.
-
- Institute of Medicine. A shared destiny: Community effects of uninsurance. Washington: National Academies Press; 2003. - PubMed
-
- Rotarius T, Trujillo A, Unruh L, et al. Uncompensated care and emergency department utilization: a local study having national implications. Health Care Manag (Frederick) 2002 Sep;21(1):1–38. - PubMed
-
- Derlet RW, Richards JR. Overcrowding in the nation’s emergency departments: complex causes and disturbing effects. Ann Emerg Med. 2000 Jan;35(1):63–8. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
