

Quality of malaria case management at outpatient health facilities in Angola
- PMID: 19954537
- PMCID: PMC2795764
- DOI: 10.1186/1475-2875-8-275
Quality of malaria case management at outpatient health facilities in Angola
Abstract
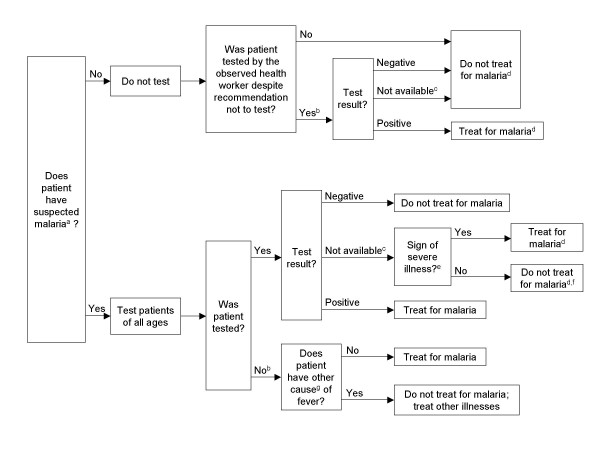
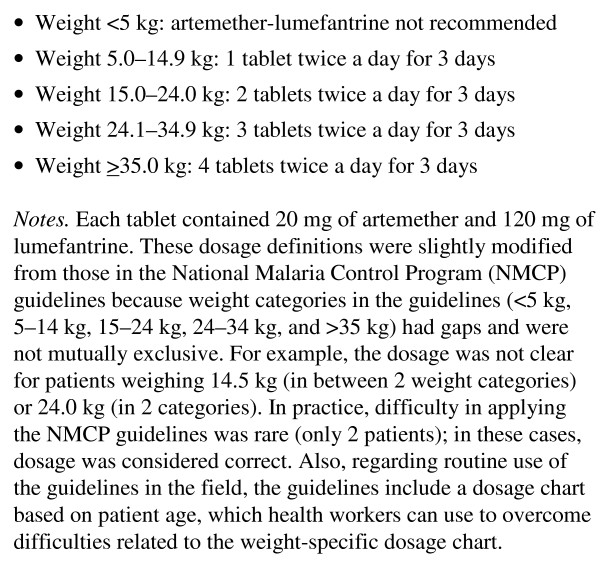
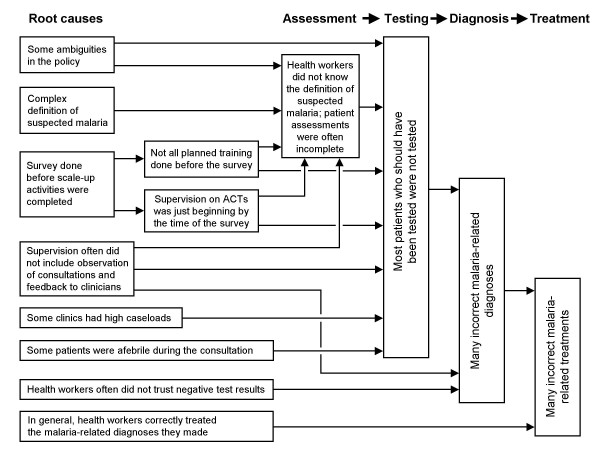
Background: Angola's malaria case-management policy recommends treatment with artemether-lumefantrine (AL). In 2006, AL implementation began in Huambo Province, which involved training health workers (HWs), supervision, delivering AL to health facilities, and improving malaria testing with microscopy and rapid diagnostic tests (RDTs). Implementation was complicated by a policy that was sometimes ambiguous.
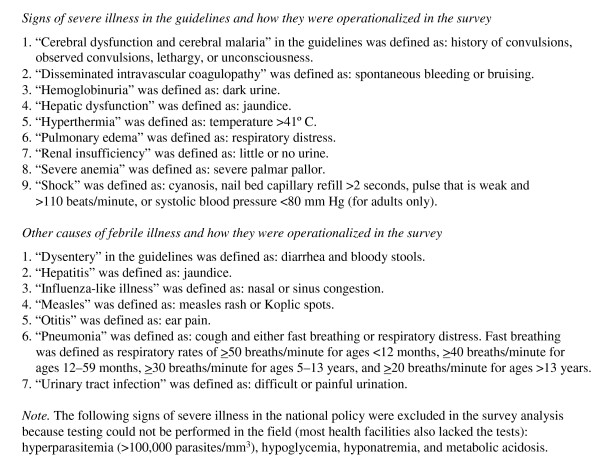
Methods: Fourteen months after implementation began, a cross-sectional survey was conducted in 33 outpatient facilities in Huambo Province to assess their readiness to manage malaria and the quality of malaria case-management for patients of all ages. Consultations were observed, patients were interviewed and re-examined, and HWs were interviewed.
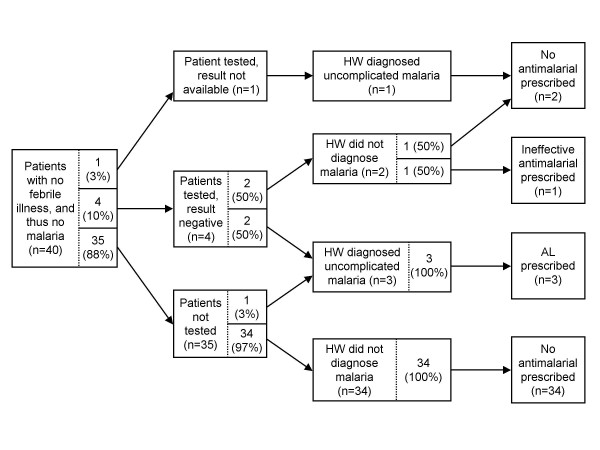
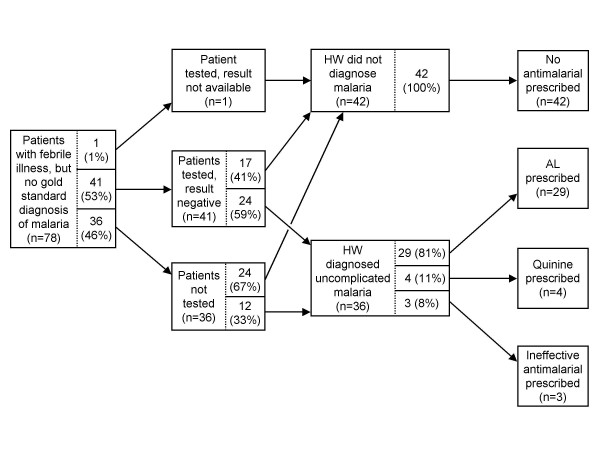
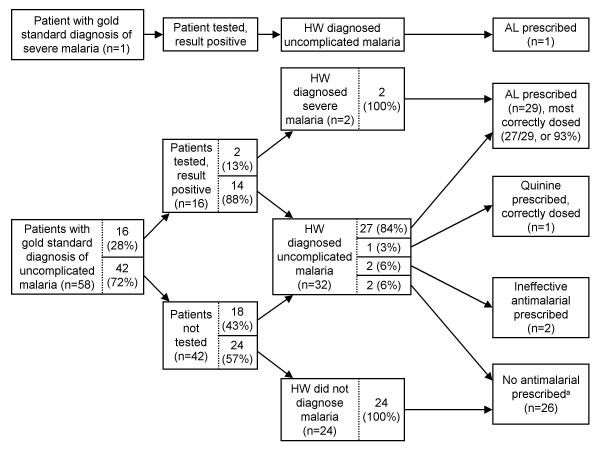
Results: Ninety-three HWs and 177 consultations were evaluated, although many sampled consultations were missed. All facilities had AL in-stock and at least one HW trained to use AL and RDTs. However, anti-malarial stock-outs in the previous three months were common, clinical supervision was infrequent, and HWs had important knowledge gaps. Except for fever history, clinical assessments were often incomplete. Although testing was recommended for all patients with suspected malaria, only 30.7% of such patients were tested. Correct testing was significantly associated with caseloads < 25 patients/day (odds ratio: 18.4; p < 0.0001) and elevated patient temperature (odds ratio: 2.5 per 1 degrees C increase; p = 0.007). Testing was more common among AL-trained HWs, but the association was borderline significant (p = 0.072). When the malaria test was negative, HWs often diagnosed patients with malaria (57.8%) and prescribed anti-malarials (60.0%). Sixty-six percent of malaria-related diagnoses were correct, 20.1% were minor errors, and 13.9% were major (potentially life-threatening) errors. Only 49.0% of malaria treatments were correct, 5.4% were minor errors, and 45.6% were major errors. HWs almost always dosed AL correctly and gave accurate dosing instructions to patients; however, other aspects of counseling needed improvement.
Conclusion: By late-2007, substantial progress had been made to implement the malaria case-management policy in a setting with weak infrastructure. However, policy ambiguities, under-use of malaria testing, and distrust of negative test results led to many incorrect malaria diagnoses and treatments. In 2009, Angola published a policy that clarified many issues. As problems identified in this survey are not unique to Angola, better strategies for improving HW performance are urgently needed.
Figures
References
-
- Barnes KI, Durrheim DN, Little F, Jackson A, Mehta U, Allen E, Dlamini SS, Tsoka J, Bredenkamp B, Mthembu DJ, White NJ, Sharp BL. Effect of artemether-lumefantrine policy and improved vector control on malaria burden in KwaZulu-Natal, South Africa. PLoS Med. 2005;2:e330. doi: 10.1371/journal.pmed.0020330. - DOI - PMC - PubMed
-
- Olumese P. Global Antimalarial Drug Policy Database. Antimalarial treatment policies for P. falciparum and P. vivax by country in WHO Africa and Easter Mediterranean Regions. http://apps.who.int/malaria/treatmentpolicies.html [May 2008 Update]. (accessed September 1, 2009).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
