

Recovery of consciousness after brain injury: a mesocircuit hypothesis
- PMID: 19954851
- PMCID: PMC2931585
- DOI: 10.1016/j.tins.2009.11.002
Recovery of consciousness after brain injury: a mesocircuit hypothesis
Abstract
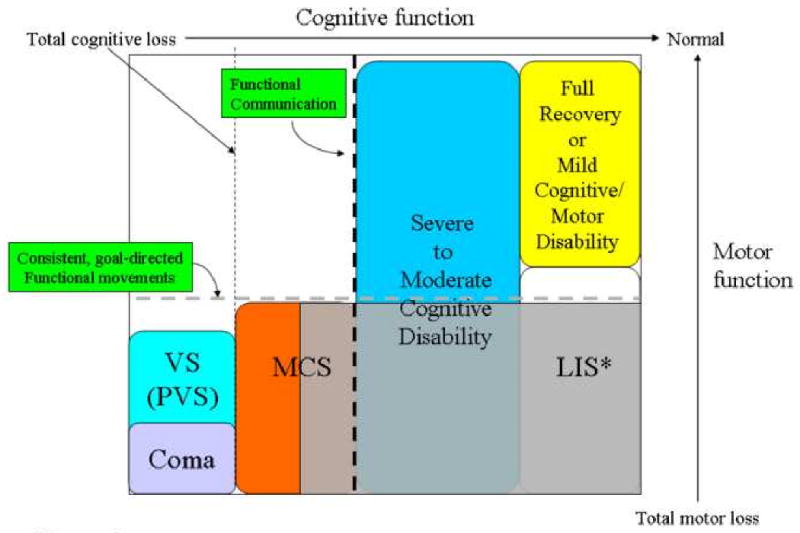
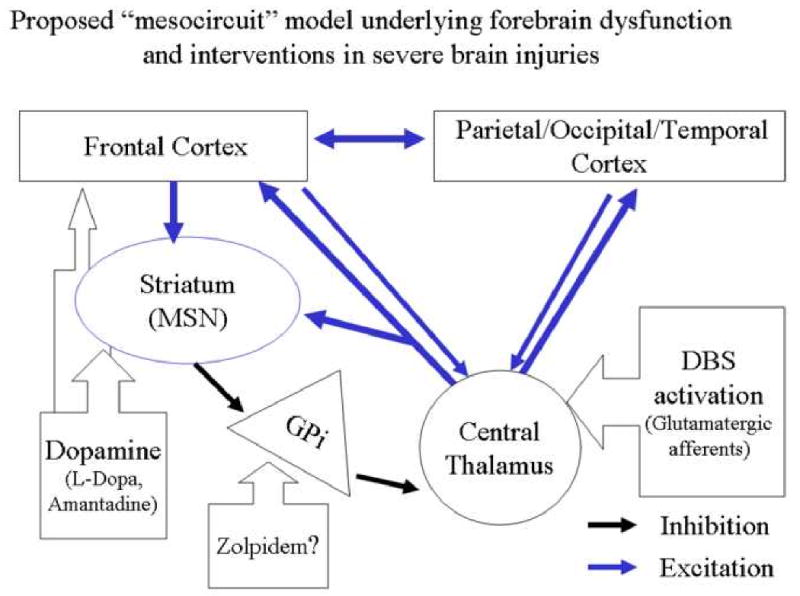
Recovery of consciousness following severe brain injuries can occur over long time intervals. Importantly, evolving cognitive recovery can be strongly dissociated from motor recovery in some individuals, resulting in underestimation of cognitive capacities. Common mechanisms of cerebral dysfunction that arise at the neuronal population level may explain slow functional recoveries from severe brain injuries. This review proposes a "mesocircuit" model that predicts specific roles for different structural and dynamic changes that may occur gradually during recovery. Recent functional neuroimaging studies that operationally identify varying levels of awareness, memory and other higher brain functions in patients with no behavioral evidence of these cognitive capacities are discussed. Measuring evolving changes in underlying brain function and dynamics post-injury and post-treatment frames future investigative work.
Copyright 2009 Elsevier Ltd. All rights reserved.
Figures
References
-
- Lammi MH, Smith VH, Tate RL, Taylor CM. The minimally conscious state and recovery potential: a follow-up study 2 to 5 years after traumatic brain injury. Arch Phys Med Rehabil. 2005;86(4):746–54. - PubMed
-
- Burruss JW, Chacko RC. Episodically remitting akinetic mutism following subarachnoid hemorrhage. J Neuropsychiatry Clin Neurosci 1999. 1999;11(1):100–2. - PubMed
-
- McMillan TM, Herbert CM. Further recovery in a potential treatment withdrawal case 10 years after brain injury. Brain Inj. 2004;18(9):935–40. - PubMed
-
- Macniven JA, Poz R, Bainbridge K, Gracey F, Wilson BA. Emotional adjustment following cognitive recovery from ‘persistent vegetative state’: psychological and personal perspectives. Brain Inj. 2003;17(6):525–33. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
