

Multiple sclerosis risk sharing scheme: two year results of clinical cohort study with historical comparator
- PMID: 19955128
- PMCID: PMC2787922
- DOI: 10.1136/bmj.b4677
Multiple sclerosis risk sharing scheme: two year results of clinical cohort study with historical comparator
Abstract
Objective: To generate evidence on the longer term cost effectiveness of disease modifying treatments in patients with relapsing-remitting multiple sclerosis.
Design: Prospective cohort study with historical comparator.
Setting: Specialist multiple sclerosis clinics in 70 centres in the United Kingdom.
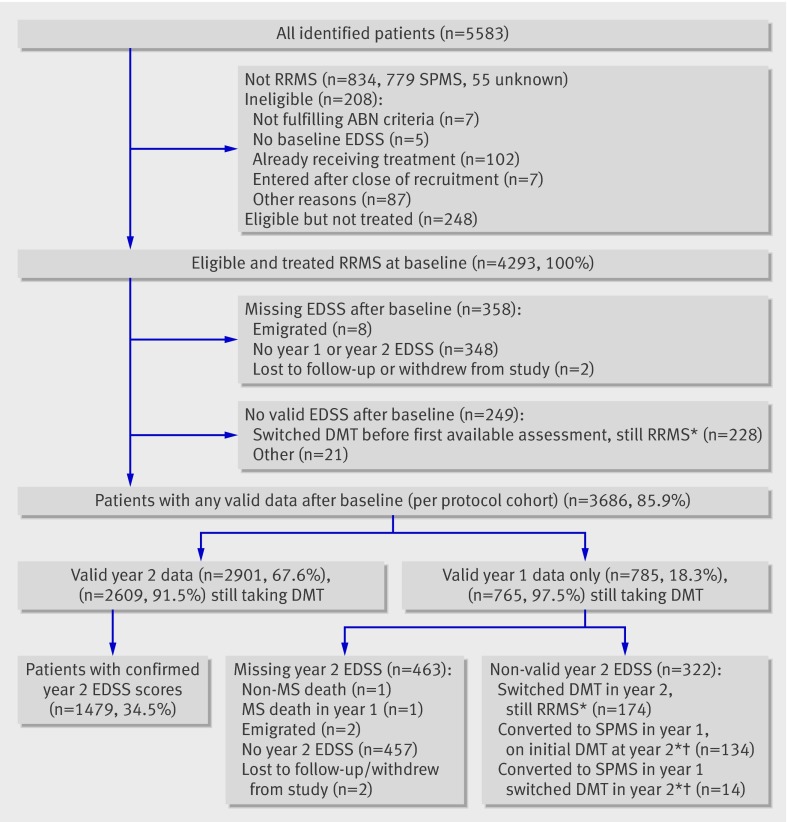
Participants: Patients with relapsing-remitting multiple sclerosis who started treatment from May 2002 to April 2005 under the UK risk sharing scheme.
Interventions: Treatment with interferon beta or glatiramer acetate in accordance with guidelines of the UK Association of British Neurologists.
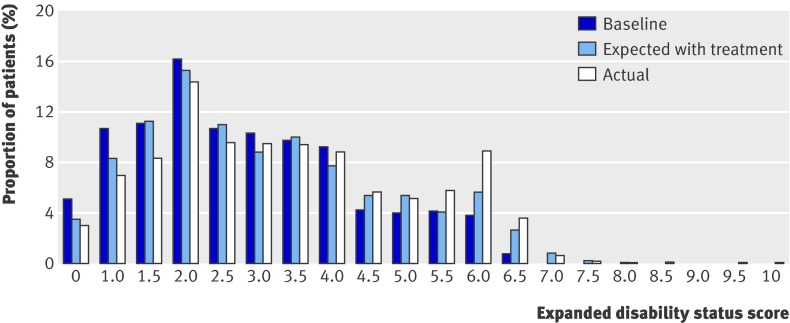
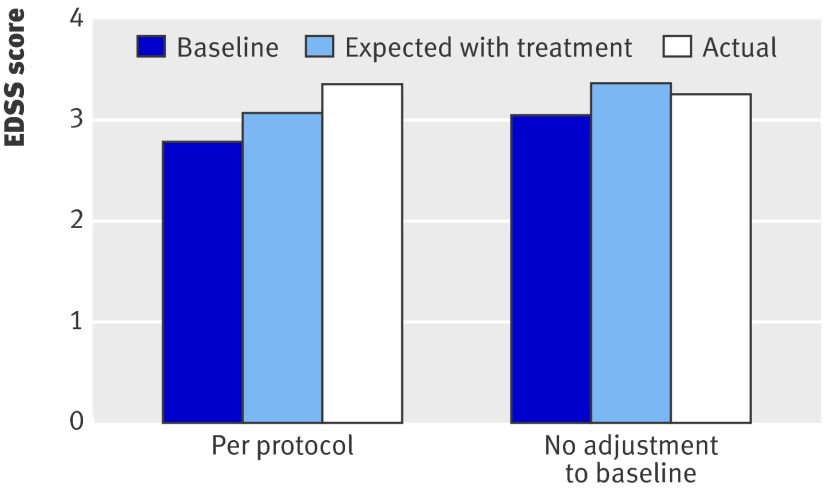
Main outcome measures: Observed utility weighted progression in disability at two years' follow-up assessed on the expanded disability status scale (EDSS) compared with that expected by applying the progression rates in a comparator dataset, modified for patients receiving treatment by multiplying by the hazard ratio derived separately for each disease modifying treatment from the randomised trials.
Results: In the primary per protocol analysis, progression in disability was worse than that predicted and worse than that in the untreated comparator dataset ("deviation score" of 113%; excess in mean disability status scale 0.28). In sensitivity analyses, however, the deviation score varied from -72% (using raw baseline disability status scale scores, rather than applying a "no improvement" algorithm) to 156% (imputing missing data for year two from progression rates for year one).
Conclusions: It is too early to reach any conclusion about the cost effectiveness of disease modifying treatments from this first interim analysis. Important methodological issues, including the need for additional comparator datasets, the potential bias from missing data, and the impact of the "no improvement" rule, will need to be addressed and long term follow-up of all patients is essential to secure meaningful results. Future analyses of the cohort are likely to be more informative, not least because they will be less sensitive to short term fluctuations in disability.
Conflict of interest statement
Competing interests: MB and JP have received support for attending international congresses from each of the four pharmaceutical companies funding the study. CD is an employee of the Department of Health and was involved in the negotiation of the original risk sharing scheme.
Figures
References
-
- National Institute for Health and Clinical Excellence. Beta interferon and glatiramer acetate for the treatment of multiple sclerosis. NICE, 2002 (Technology Appraisal Guidance No 32).
-
- Hemmett L, Holmes J, Barnes M, Russell N. What drives quality of life in multiple sclerosis? QJM 2004;97:671-6. - PubMed
-
- Kobelt G, Lindgren P, Parkin D, Francis DA, Johnson M, Bates D, et al. Costs and quality of life in multiple sclerosis. A cross-sectional observational study in the UK. Scandinavian Working Papers in Economics, 2000 (http://swopec.hhs.se/hastef/papers/hastef0398.pdf).
-
- Ebers G. Natural history of multiple sclerosis. In: Compston A, Ebers G, Lassmann H, McDonald IR, Matthews B, Wekerle H. McAlpine’s multiple sclerosis. 3rd ed. Churchill Livingstone, 1998.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous