

Warfarin sensitivity genotyping: a review of the literature and summary of patient experience
- PMID: 19955245
- PMCID: PMC2787394
- DOI: 10.4065/mcp.2009.0278
Warfarin sensitivity genotyping: a review of the literature and summary of patient experience
Abstract
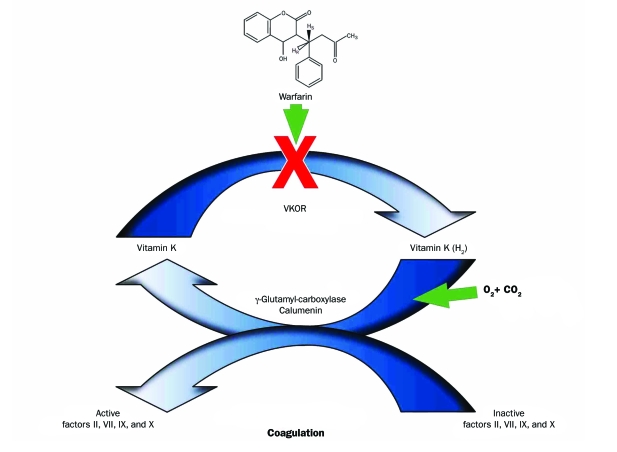
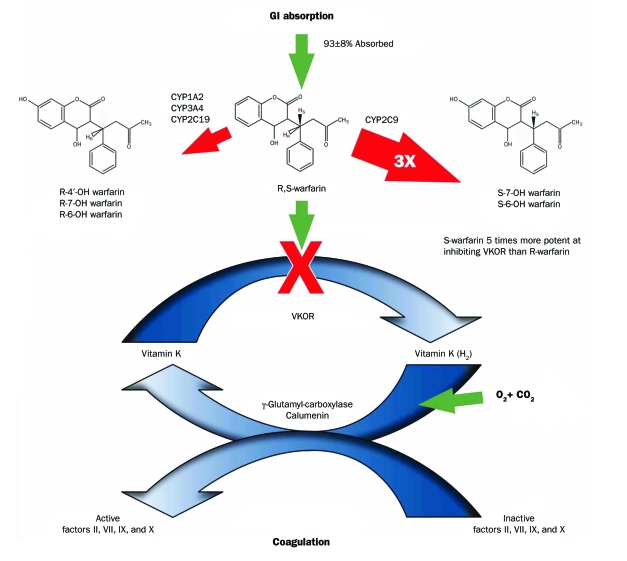
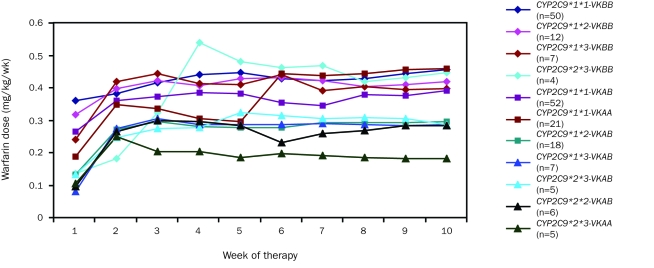
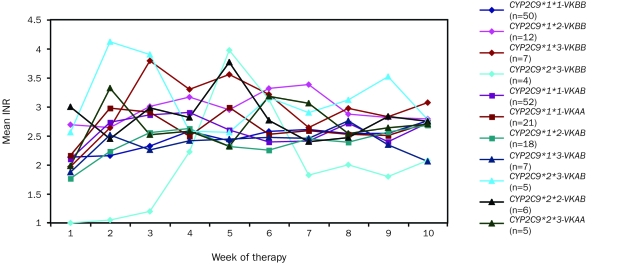
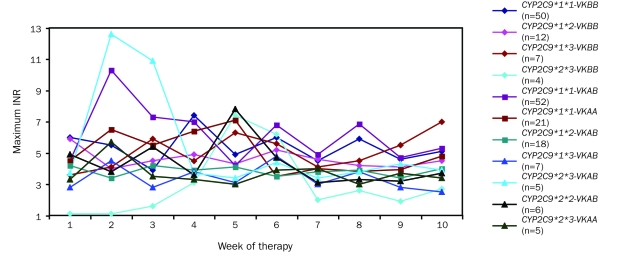
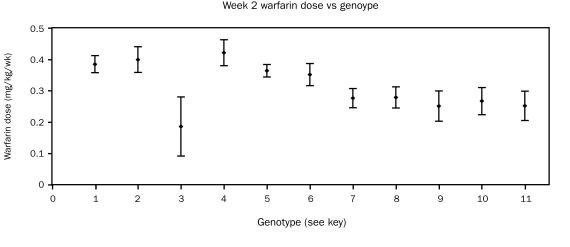
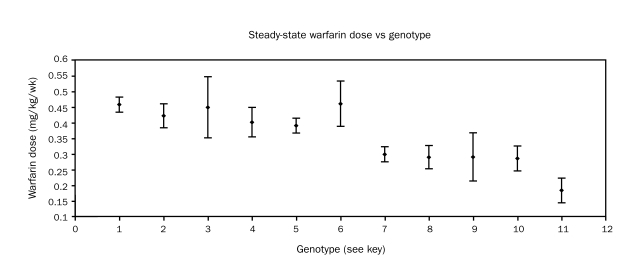
The antithrombotic benefits of warfarin are countered by a narrow therapeutic index that contributes to excessive bleeding or cerebrovascular clotting and stroke in some patients. This article reviews the current literature describing warfarin sensitivity genotyping and compares the results of that review to the findings of our study in 189 patients at Mayo Clinic conducted between June 2001 and April 2003. For the review of the literature, we identified relevant peer-reviewed articles by searching the Web of Knowledge using key word warfarin-related adverse event. For the 189 Mayo Clinic patients initiating warfarin therapy to achieve a target international normalized ratio (INR) in the range of 2.0 to 3.5, we analyzed the CYP2C9 (cytochrome P450 2C9) and VKORC1 (vitamin K epoxide reductase complex, subunit 1) genetic loci to study the relationship among the initial warfarin dose, steady-state dose, time to achieve steady-state dose, variations in INR, and allelic variance. Results were compared with those previously reported in the literature for 637 patients. The relationships between allelic variants and warfarin sensitivity found in our study of Mayo Clinic patients are fundamentally the same as in those reported by others. The Mayo Clinic population is predominantly white and shows considerable allelic variability in CYP2C9 and VKORC1. Certain of these alleles are associated with increased sensitivity to warfarin. Polymorphisms in CYP2C9 and VKORC1 have a considerable effect on warfarin dose in white people. A correlation between steady-state warfarin dose and allelic variants of CYP2C9 and VKORC1 has been demonstrated by many previous reports and is reconfirmed in this report. The allelic variants found to most affect warfarin sensitivity are CYP2C9*1*1-VKORC1BB (less warfarin sensitivity than typical); CYP2C9*1*1-VKORC1AA (considerable variance in INR throughout initiation); CYP2C9*1*2-VKORC1AB (more sensitivity to warfarin than typical); CYP2C9*1*3-VKORC1AB (much more sensitivity to warfarin than typical); CYP2C9*1*2-VKORC1AB (much more sensitivity to warfarin than typical); CYP2C9*1*3-VKORC1AA (much more sensitivity to warfarin than typical); and CYP2C9*2*2-VKORC1AB (much more sensitivity to warfarin than typical). Although we were unable to show an association between allelic variants and initial warfarin dose or dose escalation, an association was seen between allelic variant and steady-state warfarin dose. White people show considerable variance in CYP2C9 allele types, whereas people of Asian or African descent infrequently carry CYP2C9 allelic variants. The VKORC1AA allele associated with high warfarin sensitivity predominates in those of Asian descent, whereas white people and those of African descent show diversity, carrying either the VKORC1BB, an allele associated with low warfarin sensitivity, or VKORC1AB or VKORC1AA, alleles associated with moderate and high warfarin sensitivity, respectively.
Figures
References
-
- Ansell J, Hirsh J, Hylek E, et al. Pharmacology and management of the vitamin K antagonists. Chest 2008;133(suppl 6):160S-198S - PubMed
-
- Baglin TP, Cousins D, Keeling DM, Perry DJ, Watson HG. Recommendations from the British Committee for Standards in Haematology and National Patient Safety Agency. BJH 2006;136:26-29 - PubMed
-
- Flockhart DA, O'Kane D, Williams MS, et al. ACMG Working Group on Pharmacogenetic Testing of CYP2C9. VKORC1 Alleles for Warfarin Use Pharmacogenetic testing of CYP2C9 and VKORC1 alleles for warfarin. Genet Med. 2008;10(2):139-150 - PubMed
-
- Husted SE, Ziegler BK, Kher A. Long-term anticoagulant therapy in patients with coronary artery disease. Eur Heart J. 2006April;27(8):913-919 Epub 2006 Jan 9 - PubMed
-
- Singer DE, Albers GW, Dalen JE, et al. Antithrombotic therapy in atrial fibrillation: evidence-based clinical practice guidelines, American College of Chest Physicians (8th Edition). Chest 2008;133(6 suppl):546S-592S - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
