

Neuroendocrine consequences of anorexia nervosa in adolescents
- PMID: 19955768
- PMCID: PMC3731628
- DOI: 10.1159/000262540
Neuroendocrine consequences of anorexia nervosa in adolescents
Abstract
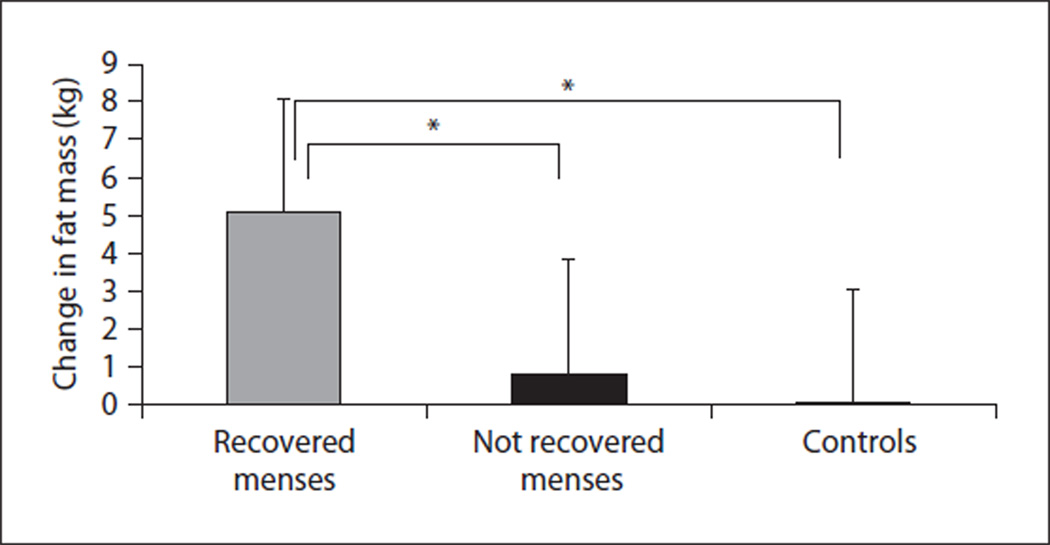
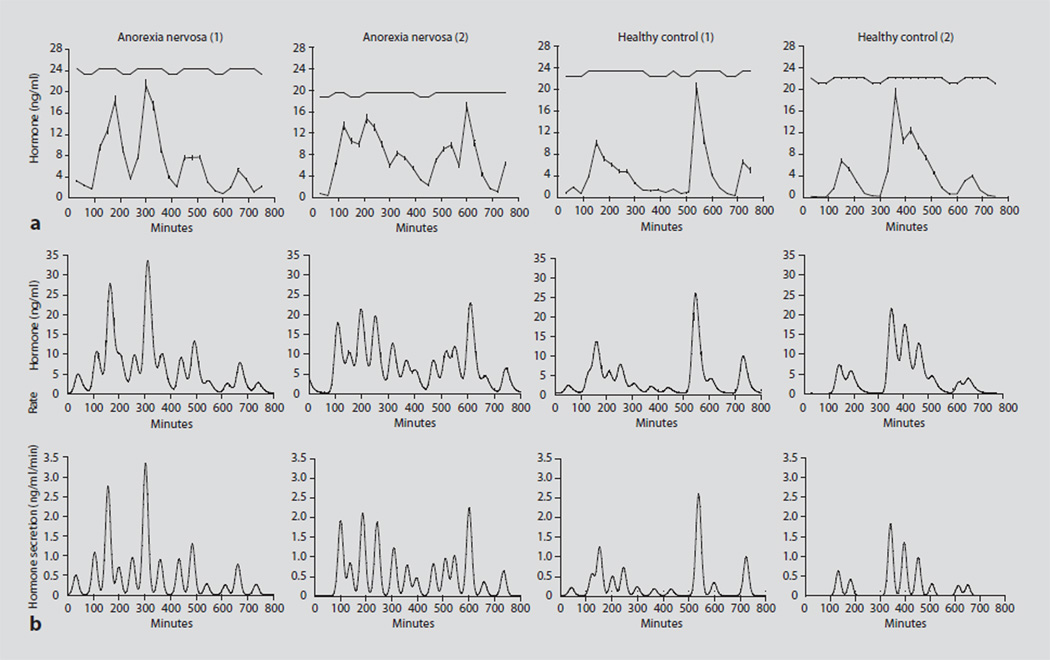
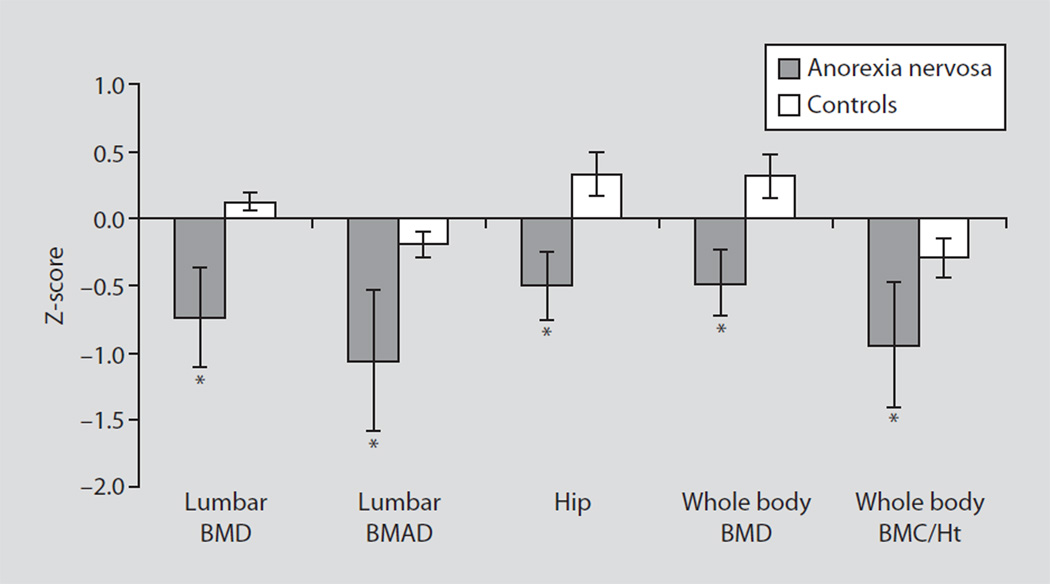
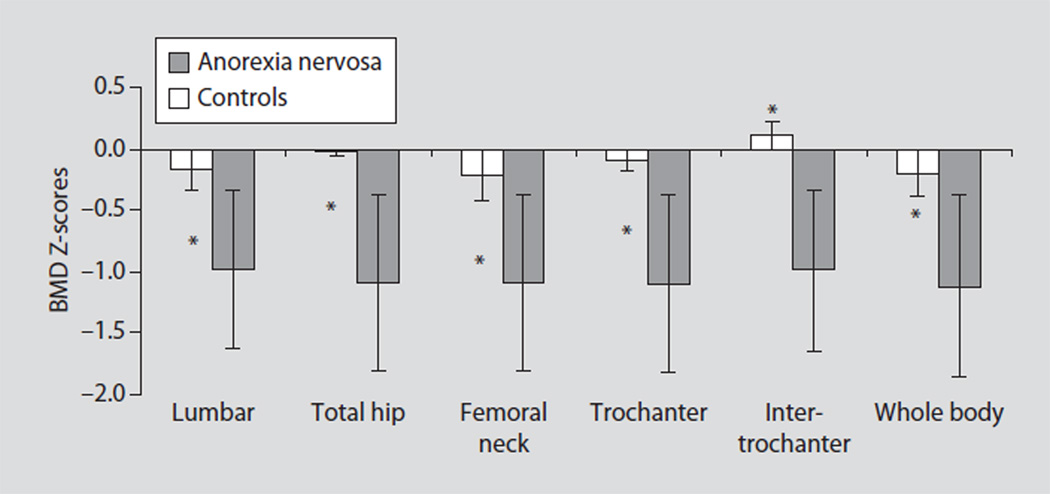
Anorexia nervosa (AN) is a condition of severe undernutrition characterized by alterations in multiple neuroendocrine axes and peptides that signal or regulate energy intake. These alterations include a state of hypogonadotropic hypogonadism, a nutritionally acquired resistance to growth hormone (GH) with low IGF-1 levels, relative hypercortisolemia, low total T3 despite normal TSH, low levels of leptin and insulin, and elevated levels of ghrelin, peptide YY (PYY) and possibly adiponectin. Although many of these changes are adaptive to low weight, they can impact bone metabolism, body composition, reproductive function and statural growth. Low bone mass is characteristic of AN in both adolescent boys and girls. In girls, sites of trabecular bone are more likely to be affected than sites of cortical bone, whereas in boys with AN, sites of cortical bone are more commonly affected. Bone microarchitecture is also affected in adolescent girls with AN, with a decrease in trabecular thickness and bone trabecular volume, and an increase in trabecular separation. Important predictors of low bone density include nutritional factors, body composition, hypogonadism, low IGF-1, elevated cortisol and PYY levels, with possible contributions of low insulin. Weight gain is associated with a stabilization of bone density, although residual deficits persist in the short term, and in some cases, long term.
Copyright 2010 S. Karger AG, Basel.
Figures

Similar articles
-
Endocrinology of anorexia nervosa in young people: recent insights.Curr Opin Endocrinol Diabetes Obes. 2014 Feb;21(1):64-70. doi: 10.1097/MED.0000000000000026. Curr Opin Endocrinol Diabetes Obes. 2014. PMID: 24275621 Free PMC article. Review.
-
Bone metabolism in adolescents with anorexia nervosa.J Endocrinol Invest. 2011 Apr;34(4):324-32. doi: 10.1007/BF03347094. Epub 2011 Feb 7. J Endocrinol Invest. 2011. PMID: 21301203 Free PMC article. Review.
-
The neuroendocrine basis of anorexia nervosa and its impact on bone metabolism.Neuroendocrinology. 2011;93(2):65-73. doi: 10.1159/000323771. Epub 2011 Jan 13. Neuroendocrinology. 2011. PMID: 21228564 Free PMC article. Review.
-
Endocrine consequences of anorexia nervosa.Lancet Diabetes Endocrinol. 2014 Jul;2(7):581-92. doi: 10.1016/S2213-8587(13)70180-3. Epub 2014 Apr 2. Lancet Diabetes Endocrinol. 2014. PMID: 24731664 Free PMC article. Review.
-
Relationships between serum adipokines, insulin levels, and bone density in girls with anorexia nervosa.J Clin Endocrinol Metab. 2007 Jun;92(6):2046-52. doi: 10.1210/jc.2006-2855. Epub 2007 Mar 13. J Clin Endocrinol Metab. 2007. PMID: 17356044
Cited by
-
Cognitive Functions in Adolescent Girls with Anorexia Nervosa during Nutritional Rehabilitation.Nutrients. 2024 Oct 10;16(20):3435. doi: 10.3390/nu16203435. Nutrients. 2024. PMID: 39458431 Free PMC article.
-
Bone mineral density in partially recovered early onset anorexic patients - a follow-up investigation.Child Adolesc Psychiatry Ment Health. 2010 Jul 8;4:20. doi: 10.1186/1753-2000-4-20. Child Adolesc Psychiatry Ment Health. 2010. PMID: 20615217 Free PMC article.
-
Neuroendocrinology of reward in anorexia nervosa and bulimia nervosa: Beyond leptin and ghrelin.Mol Cell Endocrinol. 2019 Nov 1;497:110320. doi: 10.1016/j.mce.2018.10.018. Epub 2018 Nov 2. Mol Cell Endocrinol. 2019. PMID: 30395874 Free PMC article. Review.
-
Adaptive Effects of Endocrine Hormones on Metabolism of Macronutrients during Fasting and Starvation: A Scoping Review.Metabolites. 2024 Jun 16;14(6):336. doi: 10.3390/metabo14060336. Metabolites. 2024. PMID: 38921471 Free PMC article.
-
The adolescent onset anorexia nervosa study (ANABEL): Design and baseline results.Int J Methods Psychiatr Res. 2018 Sep;27(3):e1739. doi: 10.1002/mpr.1739. Epub 2018 Aug 21. Int J Methods Psychiatr Res. 2018. PMID: 30133037 Free PMC article.
References
-
- Diagnostic and Statistical Manual of Mental Disorders. ed 3. Washington: American Psychiatric Association; 1987.
-
- Lucas AR, Beard CM, O’Fallon WM, Kurland LT. 50-year trends in the incidence of anorexia nervosa in Rochester, Minn.: a population-based study. Am J Psychiatry. 1991;148:917–922. - PubMed
-
- Misra M, Aggarwal A, Miller KK, et al. Effects of anorexia nervosa on clinical, hematologic, biochemical, and bone density parameters in community-dwelling adolescent girls. Pediatrics. 2004;114:1574–1583. - PubMed
-
- Boyar RM, Katz J, Finkelstein JW, et al. Anorexia nervosa. Immaturity of the 24-hour luteinizing hormone secretory pattern. N Engl J Med. 1974;291:861–865. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
