

Does simplicity compromise accuracy in ACS risk prediction? A retrospective analysis of the TIMI and GRACE risk scores
- PMID: 19956773
- PMCID: PMC2776353
- DOI: 10.1371/journal.pone.0007947
Does simplicity compromise accuracy in ACS risk prediction? A retrospective analysis of the TIMI and GRACE risk scores
Abstract
Background: The Thrombolysis in Myocardial Infarction (TIMI) risk scores for Unstable Angina/Non-ST-elevation myocardial infarction (UA/NSTEMI) and ST-elevation myocardial infarction (STEMI) and the Global Registry of Acute Coronary Events (GRACE) risk scores for in-hospital and 6-month mortality are established tools for assessing risk in Acute Coronary Syndrome (ACS) patients. The objective of our study was to compare the discriminative abilities of the TIMI and GRACE risk scores in a broad-spectrum, unselected ACS population and to assess the relative contributions of model simplicity and model composition to any observed differences between the two scoring systems.
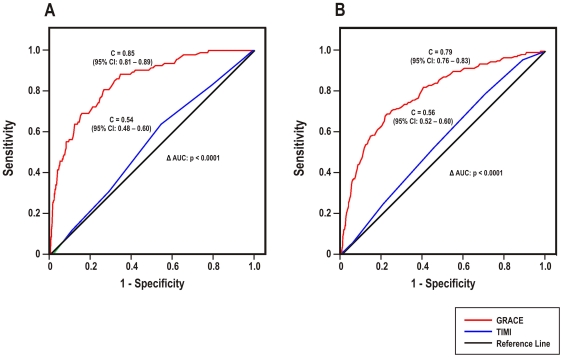
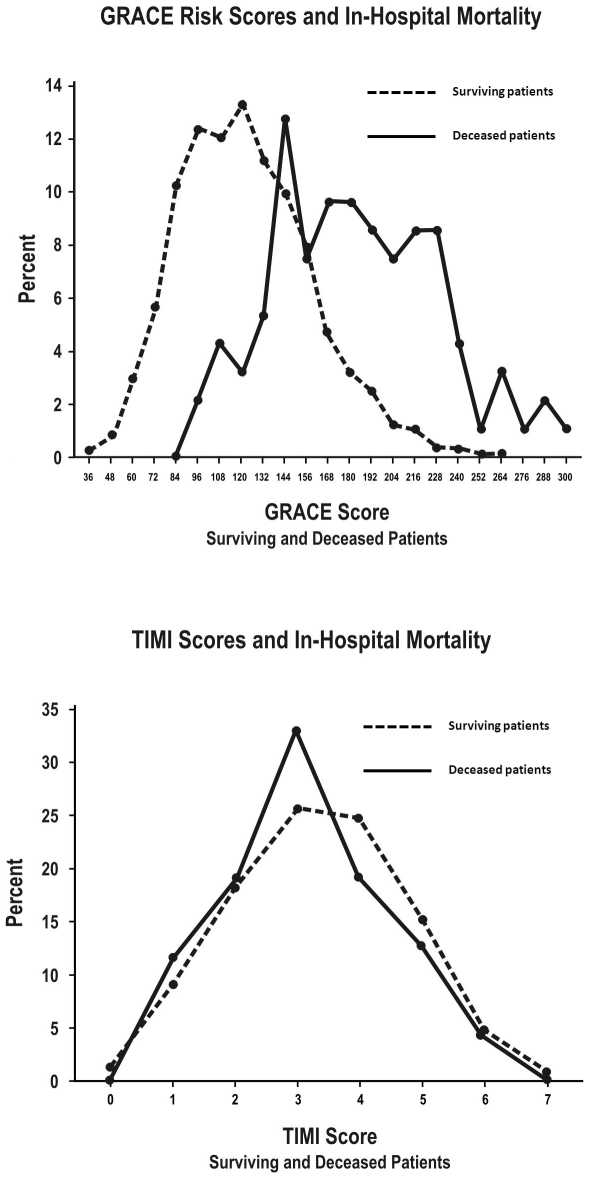
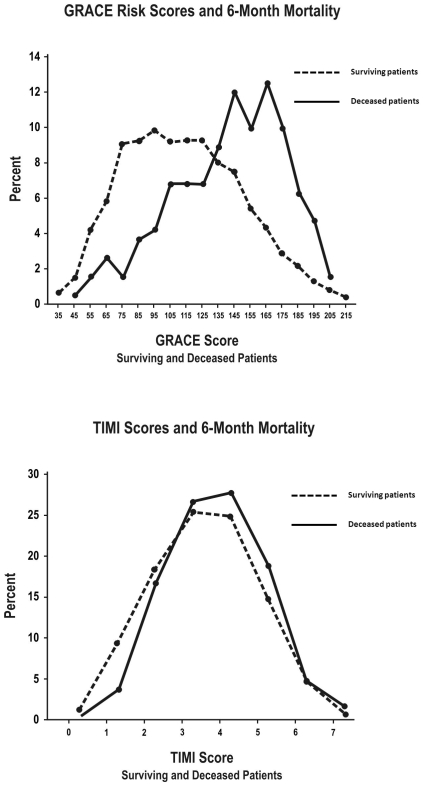
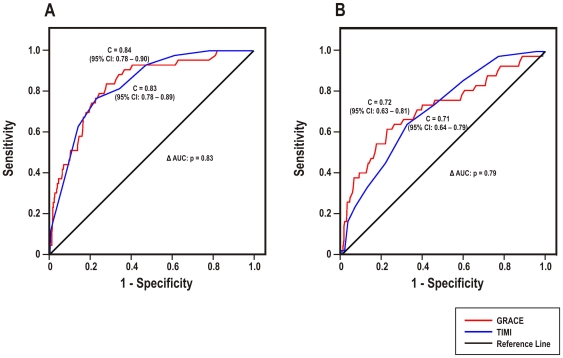
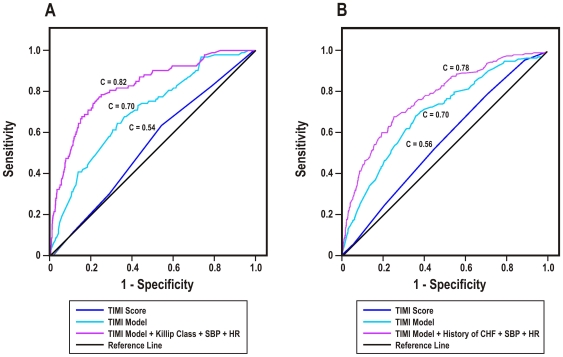
Methodology/principal findings: ACS patients admitted to the University of Michigan between 1999 and 2005 were divided into UA/NSTEMI (n = 2753) and STEMI (n = 698) subpopulations. The predictive abilities of the TIMI and GRACE scores for in-hospital and 6-month mortality were assessed by calibration and discrimination. There were 137 in-hospital deaths (4%), and among the survivors, 234 (7.4%) died by 6 months post-discharge. In the UA/NSTEMI population, the GRACE risk scores demonstrated better discrimination than the TIMI UA/NSTEMI score for in-hospital (C = 0.85, 95% CI: 0.81-0.89, versus 0.54, 95% CI: 0.48-0.60; p<0.01) and 6-month (C = 0.79, 95% CI: 0.76-0.83, versus 0.56, 95% CI: 0.52-0.60; p<0.01) mortality. Among STEMI patients, the GRACE and TIMI STEMI scores demonstrated comparably excellent discrimination for in-hospital (C = 0.84, 95% CI: 0.78-0.90 versus 0.83, 95% CI: 0.78-0.89; p = 0.83) and 6-month (C = 0.72, 95% CI: 0.63-0.81, versus 0.71, 95% CI: 0.64-0.79; p = 0.79) mortality. An analysis of refitted multivariate models demonstrated a marked improvement in the discriminative power of the TIMI UA/NSTEMI model with the incorporation of heart failure and hemodynamic variables. Study limitations included unaccounted for confounders inherent to observational, single institution studies with moderate sample sizes.
Conclusions/significance: The GRACE scores provided superior discrimination as compared with the TIMI UA/NSTEMI score in predicting in-hospital and 6-month mortality in UA/NSTEMI patients, although the GRACE and TIMI STEMI scores performed equally well in STEMI patients. The observed discriminative deficit of the TIMI UA/NSTEMI score likely results from the omission of key risk factors rather than from the relative simplicity of the scoring system.
Conflict of interest statement
Figures
References
-
- Anderson JL, Adams CD, Antman EM, Bridges CR, Califf RM, et al. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non ST-Elevation Myocardial Infarction): developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons: endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. Circulation. 2007;116:e148–304. - PubMed
-
- Antman EM, Cohen M, Bernink PJ, McCabe CH, Horacek T, et al. The TIMI risk score for unstable angina/non-ST elevation MI: A method for prognostication and therapeutic decision making. JAMA. 2000;284:835–842. - PubMed
-
- Sabatine MS, Morrow DA, Giugliano RP, Murphy SA, Demopoulos LA, et al. Implications of upstream glycoprotein IIb/IIIa inhibition and coronary artery stenting in the invasive management of unstable angina/non-ST-elevation myocardial infarction: a comparison of the Thrombolysis In Myocardial Infarction (TIMI) IIIB trial and the Treat angina with Aggrastat and determine Cost of Therapy with Invasive or Conservative Strategy (TACTICS)-TIMI 18 trial. Circulation. 2004;109:874–880. - PubMed
-
- Yan AT, Yan RT, Tan M, Eagle KA, Granger CB, et al. In-hospital revascularization and one-year outcome of acute coronary syndrome patients stratified by the GRACE risk score. Am J Cardiol. 2005;96:913–916. - PubMed
-
- Morrow DA, Antman EM, Charlesworth A, Cairns R, Murphy SA, et al. TIMI risk score for ST-elevation myocardial infarction: A convenient, bedside, clinical score for risk assessment at presentation: An intravenous nPA for treatment of infarcting myocardium early II trial substudy. Circulation. 2000;102:2031–2037. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
