

The role of steroids in the management of brain metastases: a systematic review and evidence-based clinical practice guideline
- PMID: 19957014
- PMCID: PMC2808527
- DOI: 10.1007/s11060-009-0057-4
The role of steroids in the management of brain metastases: a systematic review and evidence-based clinical practice guideline
Abstract
Question: Do steroids improve neurologic symptoms in patients with metastatic brain tumors compared to no treatment? If steroids are given, what dose should be used? Comparisons include: (1) steroid therapy versus none. (2) comparison of different doses of steroid therapy.
Target population: These recommendations apply to adults diagnosed with brain metastases.
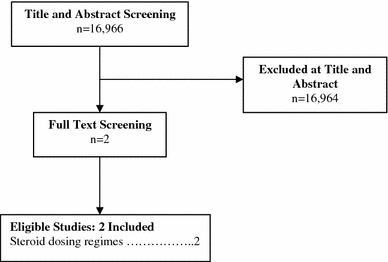
Recommendations: Steroid therapy versus no steroid therapy Asymptomatic brain metastases patients without mass effect Insufficient evidence exists to make a treatment recommendation for this clinical scenario. Brain metastases patients with mild symptoms related to mass effect Level 3 Corticosteroids are recommended to provide temporary symptomatic relief of symptoms related to increased intracranial pressure and edema secondary to brain metastases. It is recommended for patients who are symptomatic from metastatic disease to the brain that a starting dose of 4-8 mg/day of dexamethasone be considered. Brain metastases patients with moderate to severe symptoms related to mass effect Level 3 Corticosteroids are recommended to provide temporary symptomatic relief of symptoms related to increased intracranial pressure and edema secondary to brain metastases. If patients exhibit severe symptoms consistent with increased intracranial pressure, it is recommended that higher doses such as 16 mg/day or more be considered. Choice of Steroid Level 3 If corticosteroids are given, dexamethasone is the best drug choice given the available evidence. Duration of Corticosteroid Administration Level 3 Corticosteroids, if given, should be tapered slowly over a 2 week time period, or longer in symptomatic patients, based upon an individualized treatment regimen and a full understanding of the long-term sequelae of corticosteroid therapy. Given the very limited number of studies (two) which met the eligibility criteria for the systematic review, these are the only recommendations that can be offered based on this methodology. Please see "Discussion" and "Summary" section for additional details.
Figures
References
-
- Centre for Evidence-Based Physiotherapy (2009) Physiotherapy evidence database (PEDro). http://www.pedro.org.au/. Accessed Jan 2009
-
- Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. 2003;83(8):713–721. - PubMed
-
- Vecht CJ, Hovestadt A, Verbiest HB, van Vliet JJ, van Putten WL. Dose-effect relationship of dexamethasone on Karnofsky performance in metastatic brain tumors: a randomized study of doses of 4, 8, and 16 mg per day. Neurology. 1994;44(4):675–680. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
