

Benefit-risk assessment of vitamin D supplementation
- PMID: 19957164
- PMCID: PMC3062161
- DOI: 10.1007/s00198-009-1119-3
Benefit-risk assessment of vitamin D supplementation
Abstract
Current intake recommendations of 200 to 600 IU vitamin D per day may be insufficient for important disease outcomes reduced by vitamin D.
Introduction: This study assessed the benefit of higher-dose and higher achieved 25-hydroxyvitamin D levels [25(OH)D] versus any associated risk.
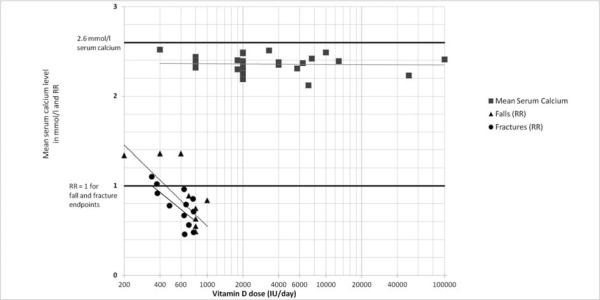
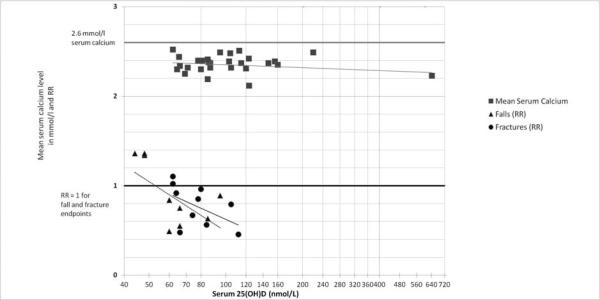
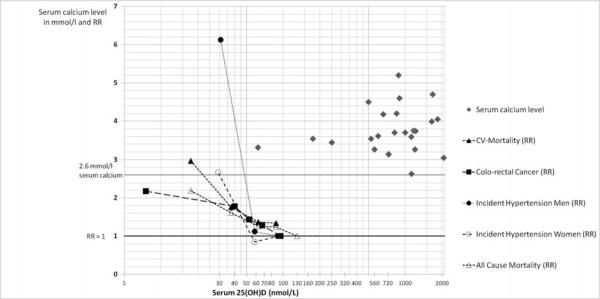
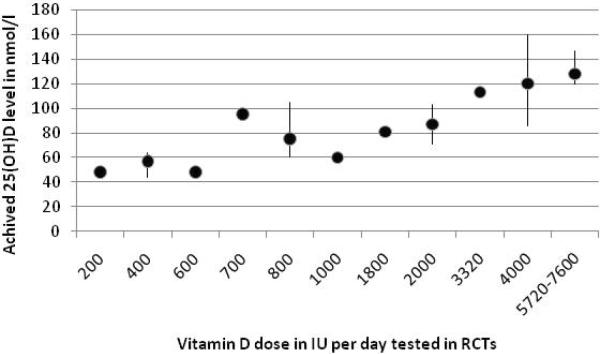
Methods and results: Based on double-blind randomized control trials (RCTs), eight for falls (n = 2426) and 12 for non-vertebral fractures (n = 42,279), there was a significant dose-response relationship between higher-dose and higher achieved 25(OH)D and greater fall and fracture prevention. Optimal benefits were observed at the highest dose tested to date for 700 to 1000 IU vitamin D per day or mean 25(OH)D between 75 and 110 nmol/l (30-44 ng/ml). Prospective cohort data on cardiovascular health and colorectal cancer prevention suggested increased benefits with the highest categories of 25(OH)D evaluated (median between 75 and 110 nmol/l). In 25 RCTs, mean serum calcium levels were not related to oral vitamin D up to 100,000 IU per day or achieved 25(OH)D up to 643 nmol/l. Mean levels of 75 to 110 nmol/l were reached in most RCTs with 1,800 to 4,000 IU vitamin D per day without risk.
Conclusion: Our analysis suggests that mean serum 25(OH)D levels of about 75 to 110 nmol/l provide optimal benefits for all investigated endpoints without increasing health risks. These levels can be best obtained with oral doses in the range of 1,800 to 4,000 IU vitamin D per day; further work is needed, including subject and environment factors, to better define the doses that will achieve optimal blood levels in the large majority of the population.
Figures
References
-
- Bischoff-Ferrari HA, et al. Prevention of nonvertebral fractures with oral vitamin D and dose dependency: a meta-analysis of randomized controlled trials. Arch Intern Med. 2009;169(6):551–61. - PubMed
-
- Dobnig H, et al. Independent association of low serum 25-hydroxyvitamin d and 1,25- dihydroxyvitamin d levels with all-cause and cardiovascular mortality. Arch Intern Med. 2008;168(12):1340–9. - PubMed
-
- Forman JP, et al. Plasma 25-Hydroxyvitamin D Levels and Risk of Incident Hypertension. Hypertension. 2007;19:19. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
