

Hemostasis during low molecular weight heparin anticoagulation for continuous venovenous hemofiltration: a randomized cross-over trial comparing two hemofiltration rates
- PMID: 19958532
- PMCID: PMC2811918
- DOI: 10.1186/cc8191
Hemostasis during low molecular weight heparin anticoagulation for continuous venovenous hemofiltration: a randomized cross-over trial comparing two hemofiltration rates
Abstract
Introduction: Renal insufficiency increases the half-life of low molecular weight heparins (LMWHs). Whether continuous venovenous hemofiltration (CVVH) removes LMWHs is unsettled. We studied hemostasis during nadroparin anticoagulation for CVVH, and explored the implication of the endogenous thrombin potential (ETP).
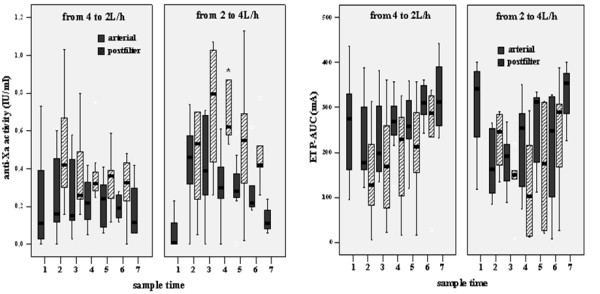
Methods: This cross-over study, performed in a 20-bed teaching hospital ICU, randomized non-surgical patients with acute kidney injury requiring nadroparin for CVVH to compare hemostasis between two doses of CVVH: filtrate flow was initiated at 4 L/h and converted to 2 L/h after 60 min in group 1, and vice versa in group 2. Patients received nadroparin 2850 IU i.v., followed by 380 IU/h continuously in the extracorporeal circuit. After baseline sampling, ultrafiltrate, arterial (art) and postfilter (PF) blood was taken for hemostatic markers after 1 h, and 15 min, 6 h, 12 h and 24 h after converting filtrate flow. We compared randomized groups, and 'early circuit clotting' to 'normal circuit life' groups.
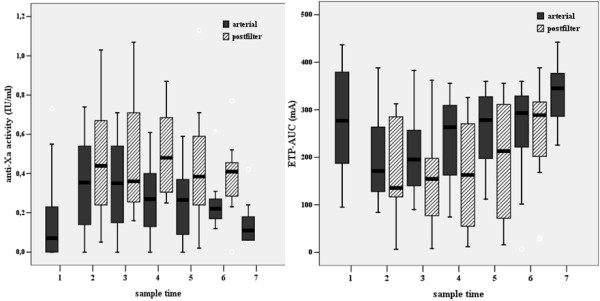
Results: Fourteen patients were randomized, seven to each group. Despite randomization, group 1 had higher SOFA scores (median 14 (IQR 11-15) versus 9 (IQR 5-9), p = 0.004). Anti-Xa art activity peaked upon nadroparin bolus and declined thereafter (p = 0.05). Anti-Xa PF did not change in time. Anti-Xa activity was not detected in ultrafiltrate. Medians of all anti-Xa samples were lower in group 1 (anti-Xa art 0.19 (0.12-0.37) vs. 0.31 (0.23-0.52), p = 0.02; anti-Xa PF 0.34 (0.25-0.44) vs. 0.51 (0.41-0.76), p = 0.005). After a steep decline, arterial ETPAUC tended to increase (p = 0.06), opposite to anti-Xa, while postfilter ETPAUC increased (p = 0.001). Median circuit life was 24.5 h (IQR 12-37 h). Patients with 'short circuit life' had longer baseline prothrombin time (PTT), activated thromboplastin time (aPTT), lower ETP, higher thrombin-antithrombin complexes (TAT) and higher SOFA scores; during CVVH, anti-Xa, and platelets were lower; PTT, aPTT, TAT and D-dimers were longer/higher and ETP was slower and depressed.
Conclusions: We found no accumulation and no removal of LMWH activity during CVVH. However, we found that early circuit clotting was associated with more severe organ failure, prior systemic thrombin generation with consumptive coagulopathy, heparin resistance and elevated extracorporeal thrombin generation. ETP integrates these complex effects on the capacity to form thrombin.
Trial registration: Clinicaltrials.gov ID NCT00965328.
Figures
Similar articles
-
Nadroparin versus dalteparin anticoagulation in high-volume, continuous venovenous hemofiltration: a double-blind, randomized, crossover study.Crit Care Med. 2000 Feb;28(2):421-5. doi: 10.1097/00003246-200002000-00022. Crit Care Med. 2000. PMID: 10708177 Clinical Trial.
-
Citrate anticoagulation for continuous venovenous hemofiltration.Crit Care Med. 2009 Feb;37(2):545-52. doi: 10.1097/CCM.0b013e3181953c5e. Crit Care Med. 2009. PMID: 19114912 Clinical Trial.
-
Predilution versus postdilution during continuous venovenous hemofiltration: a comparison of circuit thrombogenesis.ASAIO J. 2006 Jul-Aug;52(4):416-22. doi: 10.1097/01.mat.0000227733.03278.5f. ASAIO J. 2006. PMID: 16883122
-
Comparative pharmacokinetics of LMWHs.Semin Thromb Hemost. 2000;26 Suppl 1:31-8. doi: 10.1055/s-2000-9497. Semin Thromb Hemost. 2000. PMID: 11011804 Review.
-
[Continuous hemofiltration: an extrarenal filtration method used in intensive care].Ann Fr Anesth Reanim. 1991;10(4):379-89. doi: 10.1016/s0750-7658(05)80814-7. Ann Fr Anesth Reanim. 1991. PMID: 1928860 Review. French.
Cited by
-
Guideline for Reversal of Antithrombotics in Intracranial Hemorrhage: A Statement for Healthcare Professionals from the Neurocritical Care Society and Society of Critical Care Medicine.Neurocrit Care. 2016 Feb;24(1):6-46. doi: 10.1007/s12028-015-0222-x. Neurocrit Care. 2016. PMID: 26714677 Review.
-
Non anti-coagulant factors associated with filter life in continuous renal replacement therapy (CRRT): a systematic review and meta-analysis.BMC Nephrol. 2017 Feb 20;18(1):69. doi: 10.1186/s12882-017-0445-5. BMC Nephrol. 2017. PMID: 28219324 Free PMC article.
-
Low-molecular weight heparin infusion as anticoagulation for haemodialysis.Clin Kidney J. 2016 Aug;9(4):630-5. doi: 10.1093/ckj/sfw049. Epub 2016 Jun 10. Clin Kidney J. 2016. PMID: 27478610 Free PMC article.
-
Pharmacological interventions for preventing clotting of extracorporeal circuits during continuous renal replacement therapy.Cochrane Database Syst Rev. 2020 Dec 14;12(12):CD012467. doi: 10.1002/14651858.CD012467.pub3. Cochrane Database Syst Rev. 2020. PMID: 33314078 Free PMC article.
-
Clinical review: anticoagulation for continuous renal replacement therapy--heparin or citrate?Crit Care. 2011 Jan 24;15(1):202. doi: 10.1186/cc9358. Crit Care. 2011. PMID: 21345279 Free PMC article. Review.
References
-
- Hirsh J, Warkentin TE, Shaughnessy SG, Anand SS, Halperin JL, Raschke R, Granger C, Ohman EM, Dalen JE. Heparin and low-molecular-weight heparin: mechanisms of action, pharmacokinetics, dosing, monitoring, efficacy, and safety. Chest. 2001;119:64S–94S. doi: 10.1378/chest.119.1_suppl.64S. - DOI - PubMed
-
- Mismetti P, Laporte-Simitsidis S, Navarro C, Sie P, d'Azemar P, Necciari J, Duret JP, Gaud C, Decousus H, Boneu B. Aging and venous thromboembolism influence the pharmacodynamics of the anti-factor Xa and anti-thrombin activities of a low molecular weight heparin (nadroparin) Thromb Haemost. 1998;79:1162–1165. - PubMed
-
- Lim W, Dentali F, Eikelboom JW, Crowther MA. Meta-analysis: low-molecular-weight heparin and bleeding in patients with severe renal insufficiency. Ann Intern Med. 2006;144:673–684. - PubMed
-
- Isla A, Gascon AR, Maynar J, Arzuaga A, Corral E, Martin A, Solinis MA, Munoz JL. In vitro and in vivo evaluation of enoxaparin removal by continuous renal replacement therapies with acrylonitrile and polysulfone membranes. Clin Ther. 2005;27:1444–1451. doi: 10.1016/j.clinthera.2005.09.008. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
