

The impact of kidney transplantation on heart failure risk varies with candidate body mass index
- PMID: 19958864
- PMCID: PMC2804249
- DOI: 10.1016/j.ahj.2009.10.009
The impact of kidney transplantation on heart failure risk varies with candidate body mass index
Abstract
Background: The relationship of body mass index (BMI) with heart failure (HF) risk before and after kidney transplant is not well described.
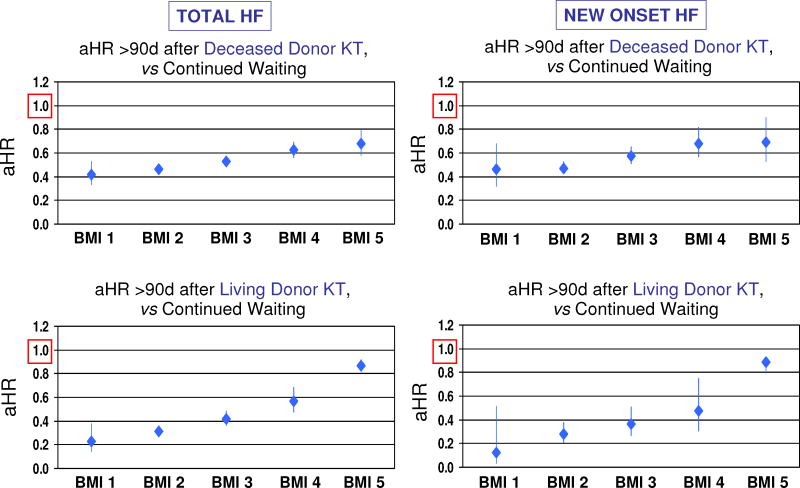
Methods: We examined United States Renal Data System records for 67,591 kidney transplant candidates (1995-2004) with Medicare insurance and BMI data at listing. Heart failure diagnoses were ascertained from Medicare billing claims. Body mass index was categorized per World Health Organization criteria. We modeled time-dependent associations (adjusted hazard ratio, aHR) of transplant with HF risk after listing compared with waiting in each BMI group by multivariable, stratified Cox regression. The time-dependent exposure variables partitioned relative risk of HF after transplant versus waiting into early (<or=90 days) and late (>90 days) posttransplant periods.
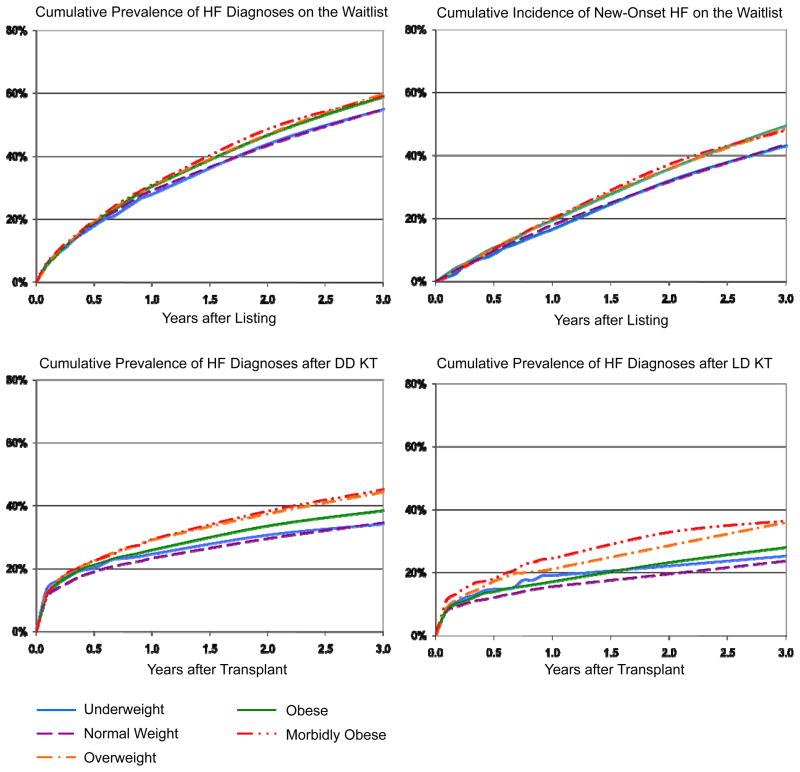
Results: The BMI distribution of listed candidates was as follows: 3.7% under, 40.4% normal, 32.0% over, 16.2% obese, and 7.7% morbidly obese weight. The prevalence of HF among patients awaiting transplant reached 57.4% by 3 years. Deceased-donor transplant was associated with increased early HF risk compared with continued waiting-aHRs ranged from 2.23 for normal-BMI to 2.82 for morbidly obese patients. However, transplant reduced the risk of HF in the late posttransplant period from 54% (aHR 0.46) in normal-BMI to 32% (aHR 0.68) for morbidly obese patients. Relative benefits were largest for normal-weight candidates who received live-donor transplants (aHR 0.31).
Conclusions: Heart failure risk improves in obese patients in the long term after kidney transplant, but not as much as for nonobese patients. There is need for close monitoring and for new strategies to reduce HF risk in obese patients before and after transplant.
Figures

References
-
- Ronco C, Haapio M, House AA, Anavekar N, Bellomo R. Cardiorenal syndrome. J Am Coll Cardiol. 2008;52(19):1527–39. - PubMed
-
- Harnett JD, Foley RN, Kent GM, Barre PE, Murray D, Parfrey PS. Congestive heart failure in dialysis patients: prevalence, incidence, prognosis and risk factors. Kidney Int. 1995;47(3):884–90. - PubMed
-
- Ferreira SR, Moises VA, Tavares A, Pacheco-Silva A. Cardiovascular effects of successful renal transplantation: a 1-year sequential study of left ventricular morphology and function, and 24-hour blood pressure profile. Transplantation. 2002;74(11):1580–7. - PubMed
-
- Wali RK, Wang GS, Gottlieb SS, Bellumkonda L, Hansalia R, Ramos E, et al. Effect of kidney transplantation on left ventricular systolic dysfunction and congestive heart failure in patients with end-stage renal disease. [see comment] Journal of the American College of Cardiology. 2005;45(7):1051–60. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
