

Variations in referral patterns to high-volume centers for pancreatic cancer
- PMID: 19959040
- PMCID: PMC4036485
- DOI: 10.1016/j.jamcollsurg.2009.09.011
Variations in referral patterns to high-volume centers for pancreatic cancer
Abstract
Background: Multiple reports have demonstrated pancreatic cancer patients undergoing surgery have superior outcomes at high-volume hospitals. This study noted trends in access to high-volume centers for pancreatic resection and identified gaps in improving access.
Study design: We performed a retrospective analysis of the Nationwide Inpatient Sample (NIS 2000 to 2005) linked to the Area Resource File (ARF). Inclusion criteria were patients with primary diagnosis of pancreatic cancer who received pancreatic resection. The primary outcomes variable was treatment at high-volume hospitals (average annual case volume greater than 20). Independent variables included age, gender, race, Charlson Comorbidity Index score, insurance status, calendar year, and region, obtained from the Nationwide Inpatient Sample; community poverty level and density of all physicians, gastroenterologists, surgeons, and radiation oncologists were data obtained from the Area Resource File.
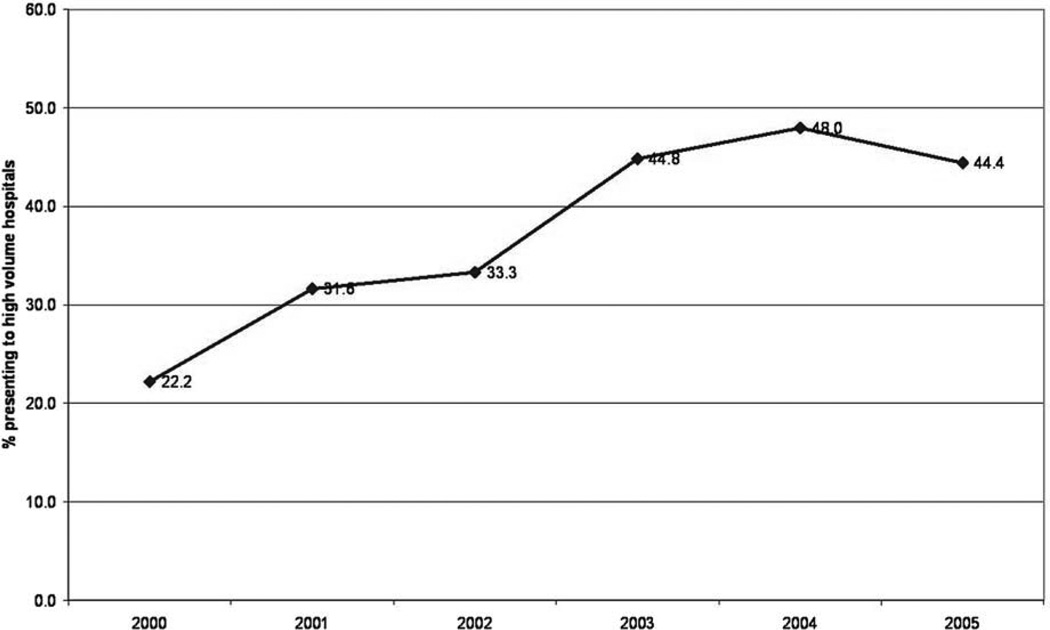
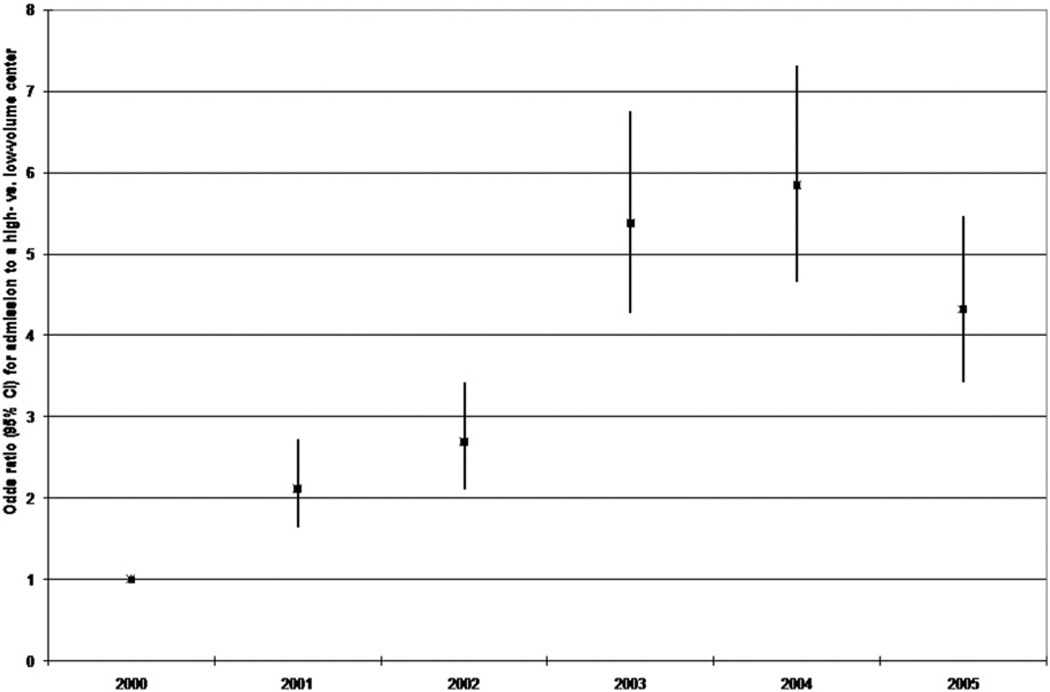
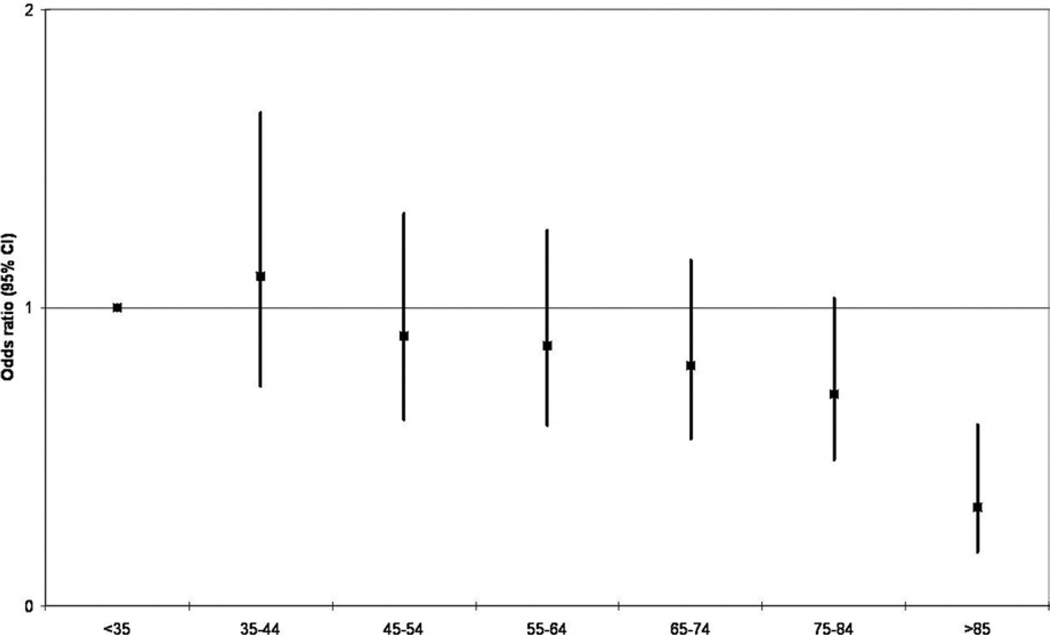
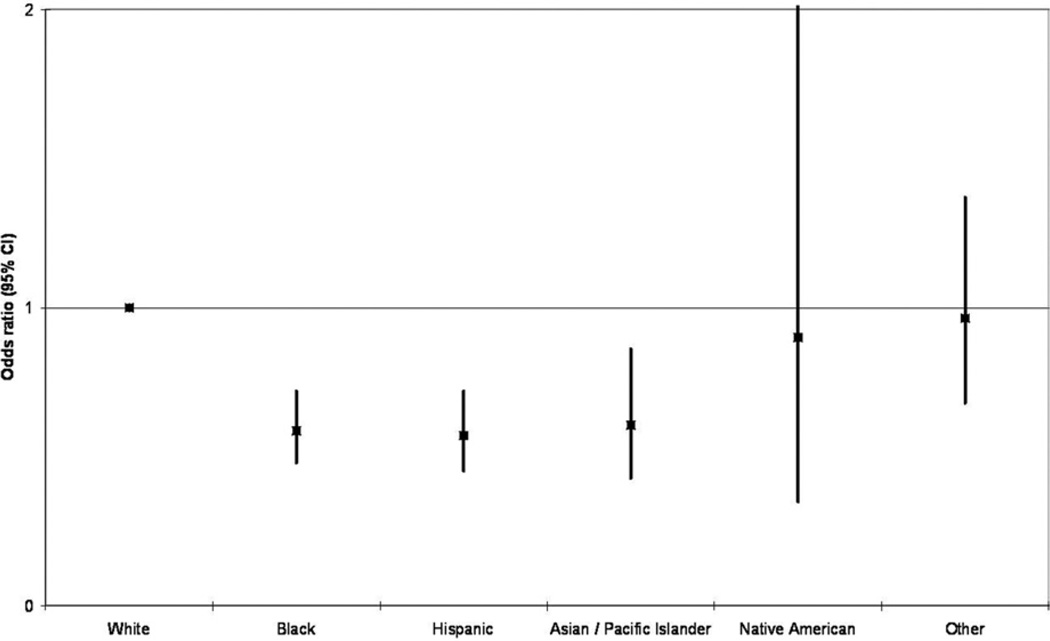
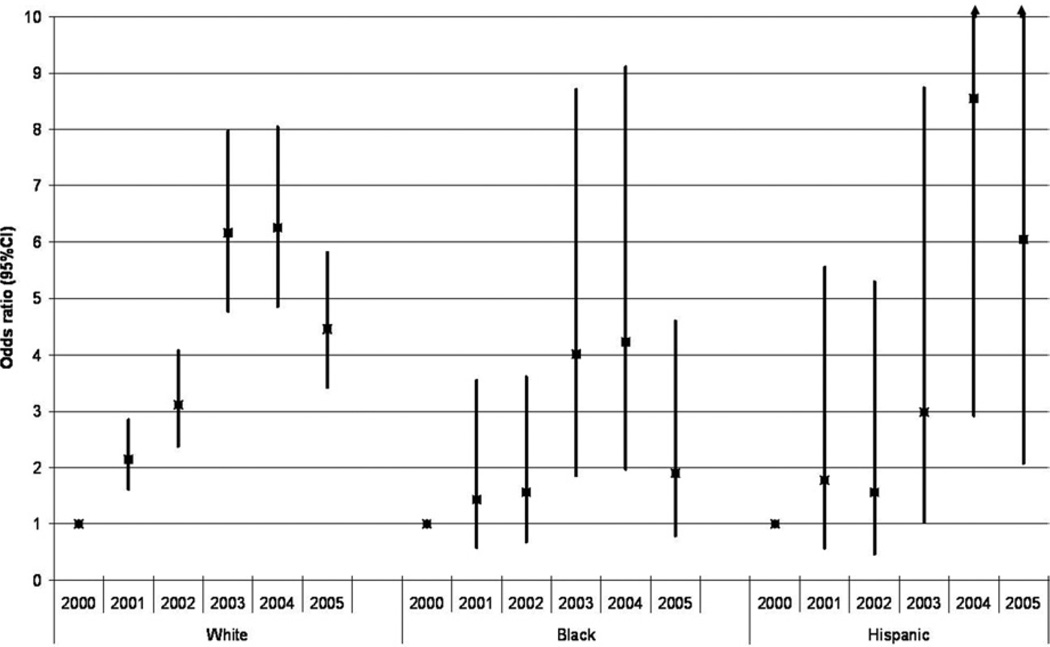
Results: A total of 8,370 patients were identified. A minority (38.51%) were referred to high-volume hospitals. A significant increase in overall referral and odds of referral to a high-volume center was observed over time (22.2% in 2000 to 44.4% in 2005). Patients referred to high-volume centers were younger (61.9 versus 63.2 years, p < 0.001) and more likely to be Caucasian (81.7% versus 73.6%, p < 0.001). Patients greater than 85 years old, African Americans, Hispanics, and Asians were less likely to be referred, relative to their younger, Caucasian counterparts (p < 0.01). The overall trend toward improved referral over time was driven by improved referral among Caucasians. In multivariate analysis, access to high-volume centers was associated with calendar year, patient age, and race. In addition, increase in density of gastroenterologists or radiation oncologists in the population was also associated with higher likelihood of referral.
Conclusions: This study demonstrated that less than half of pancreatic cancer patients are being referred to high-volume centers. Unlike referral in Caucasians, improvement in referral for minorities has not occurred.
Figures
References
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics 2008. CA Cancer J Clin. 2008;58:71–96. - PubMed
-
- Baxter NN, Whitson BA, Tuttle TM. Trends in the treatment and outcome of pancreatic cancer in the United States. Ann Surg Oncol. 2007;14:1320–1326. - PubMed
-
- Begg CB, Cramer LD, Hoskins WJ, Brennan MF. Impact of hospital volume on operative mortality for major cancer surgery. JAMA. 1998;280:1747–1751. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
